Starting solids is one of the most exciting milestones in your baby’s first year. Parents often ask me: What should I give first? Should I do purées, or jump straight into finger foods? The good news is—there isn’t one “right” way. Whether you’re beginning with spoon-fed purées or trying baby-led weaning (BLW), what matters most is offering safe, nutrient-rich foods that support your baby’s growth and development.
As a dietitian (and a mom!), I’ve put together this guide to help you feel confident when choosing those all-important first bites.
IS MY BABY READY FOR SOLIDS?
Most babies are developmentally ready around6 months, but age alone isn’t enough. Look for these readiness signs:
Baby can hold their head steady and sit with little or no support.
They show interest in food – watching you eat or reaching for your plate.
They’ve lost the tongue-thrust reflex (food doesn’t just push straight back out).
They can grasp small objects or food and bring it to their mouth.
If your baby shows these signs, you’re ready to start exploring solid foods!
WHAT NUTRIENTS DO BABIES NEED MOST?
In the first year, breastmilk or formula is still the primary source of nutrition, but solids play an important role in filling key nutrient gaps. The nutrients I prioritize when recommending first foods are:
Iron:crucial for brain development and energy (needs rise sharply around 6 months).
Zinc: supports immune function and growth.
Calcium & Vitamin D: build strong bones.
Choline & Selenium: important for brain development and antioxidant defense.
That’s why I often recommend starting with iron-rich, energy-dense foods rather than only fruits and vegetables.
PUREES VS. BABY-LED WEANING: WHICH IS BETTER?
Traditional Weaning (TW) starts with smooth purées, then progresses to mashed, then soft finger foods.
Baby-Led Weaning (BLW) skips purées, offering safe, graspable pieces of food from the start. Baby self-feeds and learns to explore textures, tastes, and independence.
Many families use a combination approach, and that’s perfectly okay! What matters is that your baby is exposed to a variety of flavors and textures, while staying safe and supported.
PALM GRASP VS. PINCER GRASP
At the start, babies use a palmar grasp (whole hand) to pick up food, so larger pieces (like avocado spears or broccoli florets) are easier for them to handle. By 9–12 months, they develop a pincer grasp (thumb and forefinger), allowing them to pick up smaller foods like beans or blueberries. Offering foods in appropriate sizes helps your baby practice motor skills while staying safe.
20 BEST STARTER FOOD FOR BABIES
Here’s a list of versatile, nutrient-packed options that can be offered as purées, mashed, or BLW-style finger foods.
Iron & Zinc-Rich Foods
Beef: slow-cooked strips (BLW) or puréed with broth.
Lamb: tender meatballs or shredded.
Chicken or turkey: shredded thigh meat or puréed with veggie stock.
Egg yolk: scrambled strips or mashed with breastmilk/formula.
Lentils: soft and mashed, or patties for BLW.
Beans (black beans, kidney beans): mashed or shaped into soft patties.
Salmon: flaked, boneless, cooked until soft.
Sardines: mashed onto toast fingers.
Tofu: soft cubes or blended with avocado.
Iron-fortified baby oatmeal: thinned with breastmilk/formula.
Healthy Fats & Energy Foods
Avocado: mashed or cut into spears (with peel left partly on for grip).
Nut butters (peanut, almond): thinned and spread thinly on toast or mixed into purées (safe introduction for allergy prevention).
Full-fat yogurt: plain, unsweetened.
Cheese: soft strips of mild cheese (e.g., mozzarella).
Starting solids is a joyful milestone, but it can feel overwhelming to decide what’s “best.” Whether you choose purées, baby-led weaning, or a mix of both, the most important thing is to focus on nutrient-rich, safe, and varied foods. Prioritize iron-rich foods from the start, introduce different textures and flavors early, and let your baby explore at their own pace.
Remember solids are about learning, not perfection. Keep mealtimes relaxed, offer family foods when possible, and always supervise closely. With variety, patience, and a positive environment, you’ll be setting the foundation for a healthy relationship with food.
Ready to help your baby thrive with Baby-Led Weaning? Enroll in Baby’s First Bites and get hands-on tips, meal ideas, and expert guidance to make mealtimes fun and nutritious.
When considering the most important nutrients for pregnant moms, many people immediately think of folic acid, iron, and perhaps Vitamin D. Similarly, when it comes to nutrients crucial for babies starting solids, iron often tops the list. While these are indeed essential, there’s another vital nutrient that deserves attention for its role in growth and development: Omega-3s, particularly DHA.
DHA is essential for brain and eye development in babies, and it supports heart health, mood stability, and cognitive function in moms. Let’s dive into why DHA is so important for both mom and baby.
OMEGA-3S
Not all omega-3 fatty acids are created equal. Among the 11 types, the three most important are ALA, EPA, and DHA.
Alpha-Linolenic Acid (ALA): ALA is the most common omega-3 fatty acid in the our diet and is primarily found in plant-based sources such as walnuts, seeds (flax, chia, hemp) and oils (canola, soybean, walnut, flaxseed). ALA is a an essential fat because it cannot be made by the body and is needed for normal human growth and development. While ALA can be converted into EPA and DHA, this conversion process is quite inefficient in humans.
Eicosapentaenoic Acid (EPA): EPA is found primarily in fatty fish and seafood. It plays a significant role in reducing inflammation throughout the body, which is crucial for preventing chronic diseases such as heart disease and arthritis. EPA also has benefits mental health, potentially reducing symptoms of depression.
Docosahexaenoic Acid (DHA): DHA is a key structural component of the brain, retina, and many other parts of the body. It is essential for brain development and function, making it particularly important during pregnancy and early childhood. DHA can be obtained either through conversion of ALA or directly from food sources rich in DHA, such as fatty fish, seafood or DHA-fortified foods.
THE CONVERSION OF ALA TO DHA
While ALA can be converted into EPA and then DHA, this conversion process, which primarily occurs in the liver, is highly inefficient, with rates reported to be less than 15%.
Additionally, studies have shown that increasing ALA intake during pregnancy does not significantly raise DHA levels in the blood (here, here). Therefore, consuming foods rich in DHA directly (or DHA supplements) is crucial for ensuring an adequate supply of this essential nutrient during pregnancy, supporting both maternal and fetal health effectively.
The active form of DHA found in foods is more beneficial than the converted form from ALA.
WHY IS DHA IMPORTANT DURING PREGNANCY?
DHA plays a crucial role in the development of a fetus’s cell membranes, particularly in the brain and retina. Ensuring adequate DHA intake during pregnancy and the first few years following birth is therefore very important. Prior to birth, the DHA required for proper fetal development is provided by placental transfer from the mother. Following birth, babies must receive DHA through breast milk, formulas fortified with DHA, or DHA supplementation (e.g., fish oil).
Brain Development:Throughout pregnancy, DHA requirements increase, especially during the third trimester. As pregnancy progresses, maternal blood volume expands, and both the placenta and the developing baby require more DHA. Therefore, DHA is required to support fetal growth and brain development, especially during the third trimester when the fetus undergoes a rapid “brain growth spurt.”
Eye Development:DHA is also essential for the development of the eyes, as it is the major fatty acid found in the retina, constituting approximately 93% of all omega-3 fatty acids. This high presence of DHA underscores its significance in eye health and visual development.
Studies indicate that during the last trimester, a fetus receives approximately 67 mg of DHA daily from the mother. This requirement increases to 70-80 mg daily during breastfeeding. The substantial demand for DHA during pregnancy and breastfeeding can deplete the mother’s DHA stores to below pre-pregnancy levels by up to 50%, and it can take months to partially replenish these levels. This depletion may pose health risks for the mother, including postpartum depression.
Research has demonstrated that sufficient DHA intake during pregnancy results in several positive outcomes for babies, such as better social behaviour, higher social development scores, enhanced verbal intelligence and reduced risk of pre-term labor, pre-eclampsia, and low birth weight.
RECOMMENDATIONS FOR PREGNANT MOMS
When it comes to recommendations for omega-3s, the guidelines can vary depending on the source. To help clarify, I’ve summarized some of the key recommendations below:
Consume 2-3 servings of low mercury fish per week, 8-12 ounces of fatty fish in total.
RECOMMENDATIONS FOR MOMS:
Those who are pregnant or breastfeeding should aim to consume 200 to 300 mg of DHA each day, which means eating 8 to 12 ounces (2 to 3 servings) per week of a variety of fish lower in mercury.
RECOMMENDATIONS FOR BABIES AND TODDLERS
The Institute of Medicine (IOM) has not established specific intake recommendations for EPA and DHA. The current recommendations for total omega-3s intake for babies aged 0-12 months is0.5g per day, and for toddlers aged 1-3 years old, the recommendation increases to 0.7g ALA per day. These targets can be met if the mother is adhering to her recommended DHA intake and breastfeeding.
Children should consume two servings of fatty fish per week.
A serving size is about:
Ages 1-3 years: 1 ounce
Ages 4-7 years: 2 ounces
Ages 8-10 years: 3 ounces
11 years and older: 4 ounces
RECOMMENDATIONS FOR CHILDREN:
Offer ultra-low mercury fish weekly, aiming for at least 2 x 1 oz. servings of DHA rich options per week.
Offer low mercury fish once every two weeks.
Offer moderately high mercury fish once every month.
Avoid high mercury fish for babies altogether.
THE FOOD SOURCE OF DHA
DHA is primarily found in fatty fish and shellfish such as salmon, herring, sardines, and trout. However, it’s important to be mindful of mercury levels, especially for pregnant women and children.
High-mercury fish like fresh/frozen tuna (big eye), tilefish, shark, swordfish, king mackerel, marlin, and orange roughy should be completely AVOIDED during pregnancy and up to 2 years old for your baby’s safety.
But don’t worry, there are plenty of low-mercury fish options packed with DHA to help you meet your nutritional needs.
ULTRA LOW-MERCURY FISH
Here are some ultra-low mercury fish (0.06 ppm of mercury or less) and rich in DHA. Offer these fish as often as you like, aiming for at least twice per week.
**The fish in bold are high in DHA with at least 0.4g DHA/100g** (reference)
Anchovies 江鱼仔
Atlantic mackerel 大西洋鲭鱼
Black sea bass 黑鲈鱼
Butterfish 奶油鱼
Catfish 鲶鱼
Clam 蛤蜊
Crawfish 小龙虾
Flounder 比目鱼
Haddock (Atlantic) 黑线鳕
Mullet 鲻鱼
Oyster 牡蛎/生蚝
Plaice 欧蝶鱼
Pollock 狭鳕
Salmon (Atlantic farmed, fresh, canned) 三文鱼
Sardine 沙丁鱼
Scallop 扇贝
Shad 西鲱
Shrimp 虾
Smelt 胡瓜鱼
Sole 鳎鱼
Squid 鱿鱼
Tilapia 罗非鱼
Trout, freshwater 淡水鳟鱼
Whiting 怀廷鱼
LOW MERCURY FISH
Offer low mercury fish (0.07 and 0.15 ppm of mercury) once every two weeks.
Atlantic croaker
Cod 鳕鱼
Crab 螃蟹
Hake 无须鳕
Herring 鲱鱼
Lobster (American and spiny) 龙虾(美洲和刺龙虾)
Pacific chub mackerel 太平洋黑鲭鱼
Perch (freshwater and ocean) 鲈鱼(淡水和海洋)
Pickerel 狗鱼
Skate 鳐鱼
Canned light tuna 罐装淡金枪鱼
Whitefish 白鱼
Buffalo fish 牛鱼
Carp 鲤鱼
Sheepshead 羊头鱼
Tilefish (Atlantic Ocean) 方头鱼(大西洋)
MODERATELY HIGH MERCURY FISH
Offer moderately high mercury fish (0.16-0.25 ppm) once every month.
Halibut 大比目鱼
Mahi mahi 鲯鳅鱼
Monkfish 安康鱼
Snapper 红鲷鱼
Spanish mackerel 西班牙鲭鱼
Striped bass 条纹鲈鱼
Weakfish / sea trout 海鲂鱼
HIGH MERCURY FISH
The following fish, with mercury levels between 0.25 and 0.45 ppm, are considered very high in mercury and should be completely avoided for babies and pregnant moms.
King mackerel 鲭王鱼
Marlin 枪鱼
Orange roughy 橙鲷
Shark 鲨鱼
Swordfish 剑鱼
Tilefish (from Gulf of Mexico) 方头鱼(墨西哥湾)
Big eye tuna 大眼金枪鱼
Bluefish (Atlantic) 蓝鱼(大西洋)
Chilean sea bass 智利海鲈鱼
Grouper 石斑鱼
Sablefish 黑鳕鱼
Tuna albacore / white tuna, canned 长鳍金枪鱼 / 白金枪鱼,罐装
Tuna albacore / white tuna, fresh/frozen 长鳍金枪鱼 / 白金枪鱼,新鲜/冷冻
Tuna yellowfin 黄鳍金枪鱼
White croaker / Pacific croaker 白石首鱼 / 太平洋石首鱼
NOT A FISH EATER OR PICKY EATER
If you find it challenging to consume fish regularly during pregnancy or you have a picky eater at home, consider omega-3 enriched eggs, which typically provide 75-100mg of DHA per serving.
FOR FORMULA-FED BABIES
For babies who haven’t started solids yet, they rely on breastmilk or formula for their DHA needs. If you’re breastfeeding, prioritize consuming DHA-rich foods to benefit both you and your baby. If formula feeding, opt for a formula with approximately 11.5 mg/100 mL of DHA, similar to the average level found in breast milk. This ensures your baby receives adequate DHA for healthy development.
EPA+DHA OR DHA ONLY
A common question is whether babies need both EPA and DHA or just DHA. While EPA is important for immune and heart health at any age, it isn’t stored in significant amounts in the brain and retina. DHA, on the other hand, is crucial for early development, especially for the brain and eyes. This is why healthcare professionals often emphasize DHA when talking about omega-3s during pregnancy and early childhood. However, since healthy fats support overall brain health and neural connectivity, it’s beneficial for babies to have adequate levels of both EPA and DHA.
IF YOU EAT FISH, DO YOU STILL NEED DHA SUPPLEMENTS?
You might wonder if consuming fish provides enough DHA, do you still need to take DHA supplements as part of your plan for nutrition during pregnancy.
Pregnant and lactating women shouldconsume 2-3 servings of a variety of fish weekly. However, even with this recommendation, you may not reach the desired DHA levels. The DHA content varies across fish species, and commonly consumed fish in Malaysia, like Indian mackerel (kembong), anchovies (ikan billis), yellow-tail and yellow-stripe scads (selar kuning), tuna (tongkol), torpedo scads (cincaru), Indian and short-fin scads (selayang), pomfret (bawal), red snapper (merah), king mackerel (tenggiri), merine catfish (jahan) and stingray (pari) have lower DHA levels compared to fish like salmon, herring, or canned white tuna.
In light of this, DHA supplementation offers a convenient solution to ensure you meet your daily DHA requirements. It simplifies monitoring your DHA intake, guaranteeing adequate levels each day, irrespective of variations in fish consumption.
Cod liver oil contains fish oil but because it also contains vitamin A, it should be AVOIDED in pregnancy.
WHAT ABOUT VEGAN?
Since fish is not a part of vegan diets and may also be excluded from certain vegetarian diets, obtaining enough DHA solely through diet can be challenging. While fish remains the best source of DHA, there are plant-based alternatives (ALA) such as walnuts and flax seeds that are rich in Omega-3 fatty acids.
Unfortunately, the conversion of ALA to DHA is inefficient, making it difficult to obtain adequate levels solely from plant-based sources. Therefore, I recommend considering an Omega-3 supplement containing at least 200 mg/day to ensure sufficient DHA intake. Additionally, for those following a vegan lifestyle, there are now vegan-friendly DHA supplements (Microalgae Oils) available, derived from algae rather than fish, providing a reliable source of this essential nutrient without compromising dietary preferences.
WHAT ABOUT ALLERGIC TO FISH?
Finned fish and shellfish are considered two different top allergens. Finned fish include species like salmon, cod, and sardines, while shellfish include shrimp, crab, and lobsters.
If your child is allergic to shellfish, it doesn’t necessarily mean they will be allergic to finned fish, as the two are biologically different. Both types of fish should be introduced EARLY and OFTEN when your child shows all signs of developmental readiness for starting solids, typically around six months.
Also, fish bones can be a choking hazard. Be sure to carefully check for bones when offering fish to your baby!
HOW TO CHOOSE AN OMEGA-3 SUPPLEMENT
There are various omega-3 supplements available on the market, when it comes to choosing an omega-3 supplement for your child, there are several important factors to consider:
1. Quality and Purity
Third-Party Testing: Ensure the fish oil manufacturer provides documentation of third-party lab results showing the purity levels of their fish oil, down to the particles per trillion level.
Manufacturing Standards: Check the quality standards the manufacturer uses. Reputable standards include the Norwegian Medicinal Standard, the European Pharmacopoeia Standard, and the Council for Responsible Nutrition’s 2006 monograph. These standards guarantee quality by setting maximum allowances for toxins.
2. Form of the Supplement
Child-Friendly Forms: Since children often find capsules difficult to swallow, look for omega-3 supplements in the form of jelly, oil, gel capsules, or chewable tablets.
Gummies Caution: Fish oil gummies are popular, but the typical dosage required to meet daily omega-3 needs might be high, leading to a high sugar intake and potential cavities. Be cautious of this and try to balance with other low-sugar options.
3. Dosage and Safety
Age Appropriateness: Choose a supplement suitable for your child’s age. Always follow the instructions on the package and do not exceed the suggested dosage.
Avoid Choking Hazards: For children under 3 years of age, avoid giving capsules as they are a choking hazard. Opt for gummies or liquid forms instead.
4. Source of the Supplement
Refined Oils vs. Fish Liver Oils: Purchase supplements made from refined oils from the flesh of fish rather than fish livers. Cod liver oils, which contain fish oil, vitamin D, and pre-formed vitamin A (retinol), can be problematic due to the fat-soluble nature of vitamin A. Excessive intake can cause serious health issues. Different brands contain varying amounts of vitamin A, so be mindful of the Recommended Dietary Allowance (RDA) for your child’s age:
1 to 2 years: 250 mcg
3 to 6 years: 300 mcg
7 to 10 years: 400 mcg
10 to 12 years: 575 mcg
BOTTOM LINE
In addition to their well-known benefits for heart health, cholesterol levels, and brain function, omega-3 fatty acids are especially important during pregnancy and infancy. DHA, a type of omega-3, is vital for the development of the fetal brain and eyes, particularly in the third trimester and early childhood.
Omega-3 fatty acids play a crucial role in promoting various aspects of overall health, including heart health, cholesterol levels, and brain function.
So often in the media we hear about the obesity epidemic and how too many children are overweight or obese. But what about those on the flip side of the coin? Some children may have difficulty eating due to selective food choices, aversions, or underlying medical concerns, making it challenging for them to consume enough calories to support their growth and development.
Being underweight is not the same as simply being thin or slender. Some children have a naturally slight build and maintain it with a well-balanced diet and physical activity.
The child’s weight can cause great worry to the parents.
IS YOUR CHILD REALLY UNDERWEIGHT?
Assessing whether your child is truly underweight is the first step in addressing any concerns you may have. It’s important not to let comments from others or comparisons with other children cause unnecessary worry.
If you’re concerned about your child’s weight, it’s best to seek professional advice from your health care professionals. Weight loss or inadequate weight gain can sometimes be a sign of an underlying medical condition, so it’s important to have your child evaluated if you’re worried.
By consulting with health care professionals, you can get a better understanding of your child’s weight status and any potential issues that may need to be addressed. This will help ensure that your child receives the appropriate support and guidance to promote their overall health and well-being.
THIN OR UNDERWEIGHT? CHECK THE GROWTH CHART
Children demonstrate their thriving and well-being through normal growth and development, which is typically assessed and monitored using growth charts. Public health nurses or pediatricians routinely plot a child’s weight, length, or height on these charts during well-visits and check-ups.
By tracking a child’s growth over time and comparing it to standardized growth curves, health care professionals can assess whether the child is growing at an appropriate rate for their age and identify any potential concerns. This allows for early intervention if there are any signs of growth faltering or deviation from the expected growth trajectory.
There are 4 nutrition indices to define nutritional status of children as measure through anthropometric measurements – body weight and height.
weight-for-age (risk for underweight)
height-for-age (risk for stunting)
body mass index (BMI)-for-age (risk for overweight)
weight-for-height (risk for wasting)
Percentiles (from 3 to 97) represent the normal window of growth we can expect for children.
The 50th percentile shows the AVERAGE – This is where most children are.
It means that below 50th percentile is lower than the average, but still normal. Above 50th percentile is above the average, but still normal too!
Here’s what the percentile values on a growth chart do mean:⠀
A 2 year old boy who places on the 48th percentile on the weight-for-age growth chart means that 52% of all the boys (same age) out there weigh more than him and 48% weigh less than him.⠀
OR
Even if your child is at the 8th percentile for his weight, meaning that 92% of kids his age weigh more than he does, if he has always been at the 8th percentile, then he is likely growing normally. It would be concerning and it might mean there was a problem with his growth if he had previously been at the 50th or 75th percentile and had now fallen down to the 8th percentile
What you should actually look at is how they progress over time on the growth chart and whether or not they’re staying on THEIR particular curve. Children who are growing normally will track their growth predictably on their own personal growth curve. Whether 48th percentile or 8th percentile, it doesn’t mean that his particular weight is good, bad, right or wrong. There is no “goal” to reach here. It just shows that body come in all shapes and forms. Some children are meant to be more petite or smaller, some are meant to be more largely built or much taller. Just look at their parents and family history as a good indicator! Genetics will win!
If time passes and you notice they’ve dropped from the 48th to the 15th percentile, that’s more of a concern! Same thing goes when it’s a big jump from the 60th percentile to the 85th percentile. That’s more of what we would call “falling off the growth curve”. It could be, of course, due to over/under-eating, malabsorption issues or some other underlying medical issue or it could be something as simple as a growth spurt.⠀
The key message here is that there’s no right or wrong percentile for your toddler! Every child has their own established growth curve. Where another child has nothing to do with where your child should be. Having a chubby or a skinny toddler does not mean they are healthy or not healthy. And trying to actively change their natural curve does a lot more harm than good.⠀
Last, the growth chart is a good indicator of your child’s overall nutritional status. If your child appears to be maintaining a usual and predictable pattern on the curve, you can rest assured that your child is getting adequate calories for normal growth.
It is not just about extra calories.
WHAT HAPPENS IF FALTERING GROWTH OR UNDERWEIGHT IS DIAGNOSED?
If faltering growth or underweight is diagnosed in a child, it can be an indicator of underlying health conditions or developmental concerns. In such cases, the doctor will typically refer the child to a pediatrician, a specialist child doctor, for further investigations.
Additionally, the pediatrician should refer the child to see a Pediatric Dietitian to assess their diet and eating routine. If this referral does not occur, it’s important for parents to advocate for their child and request a referral. They can also choose to seek assistance from a private dietitian specializing in pediatrics.
GETTING STARTED
Sometimes, parents use ineffective strategies to get their child to gain weight and grow, including negative feeding practices, in an attempt to feed them high calorie foods to boost their weight.
First, building a healthy food relationship (not just calories) is more important.
Understand the Feeding Relationship
A parent’s role is to choose whatfoods to offer,when, and where. Parents should provide healthy foods and offer regular meals and snacks.
A child’s role is to decide how muchto eat and whetheror not to eat at each meal.
Zero Pressure
Sometimes your child may refuse meals or snacks. Don’t beg, bribe or threaten your child to eat certain kinds or amounts of food.
Pressuring a child to eat can make them eat less.
Away from Distraction
Families should enjoy healthy eating together. Your child shouldn’t be singled out from the rest of the family. Everybody eats at the table together. Your child will focus on eating with fewer distractions. Turn off the TV, computer, IPad, and put toys aside around feeding time.
Stick to Mealtime Schedule
Regular meals and snacks will help your child eat enough food to grow well and be healthy. Offer food every 2-3 hours at planned times.
Offer 3 meals and 2-3 snacks each day.
Watch Empty Calories
Limit foods like sugary drinks, candies, potato chips and donuts. These foods don’t help children grow well.
Set Mealtime Boundaries
Set some table rules at meal times such as “everyone stays at the table until dad/mum’s finished”, even if your child doesn’t want to eat what you’ve served. Because they are sitting with food in front of them, they may end up picking at it! This is useful if your child wants to rush off and play rather than eat. But don’t force or nag them to eat. You’re just asking them to stay at the table. You don’t want to turn mealtimes into a battle.
Avoid Filling Up on Fluids
Drinking too many fluids like milk and juice may make a child less hungry for meals and snacks.
Serve no more than 2-3 cups of milk each day. Limit fruit juice to 0-1/2 cup each day.
Read Label
Limit foods and drinks labelled “light”, “low fat”, “fat-free”, “low calorie” or “sugar-free”.
Watch Your Languages
Watch your language and conversation around body size and shapes. If you talk about people being fat, on a diet, over-eating, or you are watching your own weight by counting calories or you obsess over food labels and your own body shape, then a child picks up on this quickly. Children mirror a parent’s pattern and chatter. Catch yourself out and avoid this kind of chatter, especially if your child has suddenly started eating less and is starting to lose weight, they may have started dieting because of this unhealthy conversation.
CAN FOOD INTOLERANCE AFFECT MY CHILD’S WEIGHT?
Yes, food intolerance can potentially contribute to a child’s low weight if it leads to inadequate food intake or nutrient absorption. For example, lactose intolerance may necessitate restricting certain dairy products, which could impact a child’s overall nutrient intake if suitable alternatives are not provided.
It’s crucial to ensure that any foods omitted from a child’s diet due to intolerance are replaced with suitable alternatives to prevent nutritional deficiencies. Unfortunately, many children may not receive proper guidance on how to replace missing nutrients when certain foods are eliminated from their diets.
Consulting with a Pediatric Dietitian can provide tailored dietary advice to ensure that your child receives all the necessary nutrients for growth and development, even in the presence of food intolerances. A dietitian can help identify suitable alternatives and ensure that the child’s diet remains balanced and nutritious.
CAN CONSTIPATION CONTRIBUTE TO POOR APPETITE?
Yes, constipation can contribute to poor appetite in children because they may feel full or uncomfortable, leading to a decreased desire to eat.
To help alleviate constipation and improve appetite, you can incorporate the following strategies:
Offer fruits and vegetables at least five times a day. These foods are rich in fiber, which can aid digestion and alleviate constipation.
Ensure your child drinks at least eight glasses of water each day, and even more in warmer weather. Staying hydrated can help soften stool and promote regular bowel movements.
Replace white versions of breakfast cereals, pasta, rice, and bread with wholemeal or wholegrain versions. Whole grains are higher in fiber, which can help regulate bowel movements and prevent constipation.
Implementing these dietary changes can help manage constipation and promote a healthy appetite in children. Additionally, I have another blog on managing constipation, you can read here.
FOODS TO GAIN WEIGHT
Parents and caregivers often ask: “How can I help my underweight child gain weight with calorie-dense foods?” or“How many calories should my children be eating?”.
They are usually struggling with knowing which foods to feed their child to help them gain weight.
Every Bite Count
Every bite of food and every gulp of liquid can make a contribution to your child’s ability to gain weight and grow. Offer foods high in calories and rich in nutrients at every meal and snack.
Make some simple switches to double up their energy intake without making them eat more.
[sg_popup id=”189025″ event=”click”][/sg_popup]
[sg_popup id=”189025″ event=”click”][/sg_popup]
THE RIGHT WAY TO INCREASE CALORIES
In Malaysia, it’s easy to find highly processed sugary snacks, many are packed with empty calories lacking in essential nutrients like protein, fiber, vitamins, and minerals.
When aiming to increase your child’s calorie intake, it’s crucial to prioritize nutrient-rich foods. Here’s what to look for:
1. High Protein
Protein plays a crucial role in supporting growth hormone levels and may aid in increasing height and weight, especially in children who are extremely picky eaters or experiencing stunted growth. Complete protein sources contain all the essential amino acids necessary for child growth. These include:
Lean meats
Poultry
Fish
Eggs
Milk
Cheese
Yogurt
Soybeans
Quinoa
However, even if a protein source is incomplete, you can still combine different sources strategically throughout the day to ensure your child receives all the necessary amino acids.
Here are some examples of high-calorie protein sources:
Eggs
Greek yogurt
Cottage cheese
Meat, poultry, and fish
Tofu
Beans and other legumes
Hemp seeds
Nutritional yeast
Protein powders (which may be beneficial in some cases, but it’s important to choose high-quality brands)
2. Healthy Fats
Healthy fats are essential for providing concentrated calories, supporting brain function, and aiding in the absorption of fat-soluble vitamins like A, D, E, and K. Including a good source of healthy fats in each meal is ideal for overall health. Here are some examples of healthy fats:
Avocado
Coconut, coconut oil, and coconut milk
Olive oil
Full-fat dairy products such as cheese, milk, yogurt, and kefir
Fatty fish like salmon, tuna, sardines, and mackerel
Nut and seed butters (great for adding to smoothies)
Chia seeds and flaxseeds
Tahini and sesame seeds
Butter and ghee
Good quality mayonnaise
3. Iron
It’s well known that iron deficiency leads to a failure to grow at normal rates, and with the high rates of iron deficiency even in Malaysia, focusing on iron (and vitamin C for absorption) is critical for underweight/short stature children.
Examples of high calorie iron rich foods include:
Beef
Chicken
Fortified Oats
Beans and lentils
Tofu
Dried apricots
4. Calcium and Vitamin D
Calcium and Vitamin D are vital for bone growth, especially in growing children. Ensuring an adequate intake of calcium is particularly important for vegan children to support their overall health and growth. Here are some high-calorie sources of calcium and Vitamin D:
Full-fat yogurt
Full-fat cheese
Salmon, rainbow trout, sardines (also rich in Vitamin D)
White beans
Soybeans (edamame)
Egg yolks
5. High Fibre
In addition to these sources, quick forms of calories from high fibre starchy fruits and vegetables are essential for providing energy from unprocessed foods in your child’s diet. Some examples include:
Sweet potato
Potato
Winter squash
Banana
Grapes
Pineapple
Goji berries
Raisins, prunes, dates
SOMETHING TO KEEP IN MIND
Here are some tips to effectively increase your child’s calorie intake:
1. Customize Meals
Prepare meals with added calories specifically for your child without altering the entire family’s diet. For instance, add extra oil or butter to one serving of pasta, spread more nut butter on your child’s bread, serve whole milk with meals, or mix in additional cream and maple syrup to oatmeal.
2. Opt for Individual Servings
Purchase smaller packages and individual servings of foods to minimize waste while experimenting with different options.
3. Consider Portion Size
Recognize that young children have smaller stomachs and may not be able to consume large volumes of food. Choose foods from above that offer higher calorie in smaller portions.
For example, while hummus provides 25 calories per tablespoon, cream cheese offers 50 calories per tablespoon, and peanut butter provides 100 calories per tablespoon. If your child consumes small amounts, opt for calorie-dense options like cream cheese or peanut butter when serving with toast.
4. Maintain Balance
Ensure a balanced diet by incorporating high-calorie foods (that your child actually enjoy) alongside nutritious options. For example, if your family is having grilled chicken for dinner, pair it with high-calorie side dishes like sweet potato fries and steamed broccoli. Then, add extra butter to the portions for the child who requires additional calories.
ACTIVE LIFE
Give your child more time to be active. Being active can make children hungrier for meals and snacks. Limit screen time, like watching TV and using other electronics. Read this post to learn how to increase physical activity level of your child.
BLUR PIC
I’ve also got another free FOODS TO GAIN WEIGHT guide you can use for your children to get you started so you can start feeling better about every bite your child takes.
BOTTOM LINE
If you’re concerned about your child’s weight but they haven’t been diagnosed as underweight, it is important to discuss your concerns with their pediatrician. The pediatrician can review their growth history and determine if further evaluation or dietary adjustments are necessary.
Remember, the need for high calorie nutritious foods may be short term, and it’s essential to prioritise your child’s overall health and well-being. While it’s important for your child to eat, at the same time not to turn mealtime into a battle or power struggle. Creating a positive eating environment can help promote healthy eating habits in the long run.
If you’re struggling to put weight on your child or worried about their nutrition, consider seeking guidance from a pediatric dietitian. A dietitian can work with you to develop a tailored plain to meet your child’s nutritional needs and ensure they are receiving the necessary nutrients for growth and development. Ultimately, the goal is to have a healthy, happy, and confident child.
Are you worried about your thin child? Are you thinking that you might want some one-on-one nutrition counselling, either for you, or your baby or child? Check out my one-on-one nutrition counselling services here.
Undoubtedly, introducing nuts to a baby can be scary, as they pose both a choking hazard and rank among the top nine allergens.
However, introducing nuts to your baby between the ages of 6 and 12 months can actually help lower their chances of developing an allergy. So, how can you safely introduce nuts to your baby?
WHAT CAUSES AN ALLERGY
An allergy occurs when the immune system erroneously recognizes a protein in a specific food as a potential threat. Subsequently, the immune system becomes activated and releases substances like histamines to combat this perceived danger. This immune response triggers inflammation, which results in the symptoms of an allergic reaction.
BENEFITS OF NUTS FOR BABY
Nuts offer a wealth of nutrients and health benefits, and there are numerous ways to include them in a baby’s diet.
Different nuts have different nutrient profiles, but generally, they are rich in fats crucial for a baby’s growth and development. Additionally, they provide essential protein for muscle growth and tissue repair, along with fiber to support a healthy digestive system. Nuts are also a source of important micronutrients such as calcium, iron, folate, vitamin E, zinc, and more.
WHEN TO INTRODUCE PEANUTS AND OTHER NUTS TO BABY
Back in 2000, parents were advised to avoid the introduction of allergenic foods for the first 1 to 3 years of life, with the belief that this would reduce the risk of developing allergies. However, recent research has shed light on this matter, revealing that delaying the introduction of allergenic foods not only fails to provide protection against allergies but can actually raise the risk of developing them.
A significant study called the LEAP study, conducted in England from 2006 to 2014, focused on infants at high risk of developing peanut allergies, including those with severe eczema, an egg allergy, or both. This study found that babies who were introduced to peanuts before the age of one and consumed them regularly in their diet had an 86% reduction in peanut allergy compared to children who avoided peanut.
Specifically, the group of children who avoided peanuts had a 17% incidence of peanut allergy, while the group that regularly included peanuts had a substantially lower rate of 3%. These findings underscore the importance of early and consistent introduction of allergenic foods like peanuts to reduce the risk of allergies in high-risk infants.
These guidelines recommend the introduction of allergenic foods at around 6 months of age, when babies are developmentally ready for solids (not before 4 months), and that all babies should have these foods by 12 months. This includes babies at high risk of allergy, unless an allergy to that particular food has already been confirmed.
Furthermore, once allergenic foods are introduced, it is beneficial to continue offering them regularly, approximately twice a week, as this practice helps in maintaining tolerance and reducing the risk of developing allergies.
WHAT NUTS CAN BE INTRODUCED TO BABY
PEANUTS VS TREE NUTS
Peanuts and tree nuts, despite both being categorized as ‘nuts,’ do not share a botanical relationship and originate from distinct plant families. Surprisingly, peanuts aren’t true nuts; they belong to the legume family, such as soybeans, chickpeas or kidney beans. Interestingly, most individuals with a peanut allergy can typically consume other legumes safely.
Peanuts
Almonds
Brazil nuts
Cashews
Chestnuts
Hazelnuts
Macadamia nuts
Pine nuts
Pecans
Pistachios
Walnuts
We know that peanuts are not related to tree nuts, so most people tend to be allergic to either peanuts OR tree nuts. However, approximately 1 in 3 individuals with a nut allergy are allergic to both peanuts and tree nuts.
It’s now known that there is some cross-reactivity can occur between different foods, as well as between pollen and certain foods or latex and certain foods. So, having a tree nut allergy doesn’t necessarily indicate an allergy to all types of tree nuts, but it significantly increases the risk of being allergic to others. For this reason, each type of nut needs to be introduced separately, ideally leaving 2-3 days between each one.
NUT BUTTERS
You have the option to prepare your own nut butter or purchase a commercially available brand of any of the nuts listed above. If opting for a store-bought variety, ensure that it is free from any additives like sugar, salt, oils, or preservatives. It should only contain the specific nut you intend to introduce.
After individually introducing each type of nut to your baby, using mixed nut butter can be a convenient method to continue exposing your baby to a variety of nuts simultaneously, rather than incorporating each nut separately. This approach simplifies the process of diversifying your baby’s nut consumption while ensuring they receive a broad range of nut-related nutrients.
A useful tip for nut butter:If your nut butter is too thick and clumpy, you can transfer a small amount to a microwave-safe bowl and heat it in 20-second intervals, stirring each time, until it becomes slightly warm. The heat will aid in smoothing out the nut butter and making it thinner in consistency.
GROUND OR FINELY CHOPPED NUTS
Another way to introduce nuts to your baby is by finely grinding them and then sprinkling them on top of pureed foods, oat cereal, avocado, banana, or other solid foods. To grind the nuts, you can take a small handful and pulse them in a blender or food processor until they are finely chopped. It’s essential to check the size of the nuts while pulsing every 20 seconds to avoid turning them into a paste or nut butter. Alternatively, you can finely chop a small quantity of nuts on a cutting board. Once you have the finely chopped nuts, you can sprinkle them onto your baby’s food, leave them as they are, or stir them in for added texture and flavor.
ARE NUTS A CHOKING HAZARD FOR BABY?
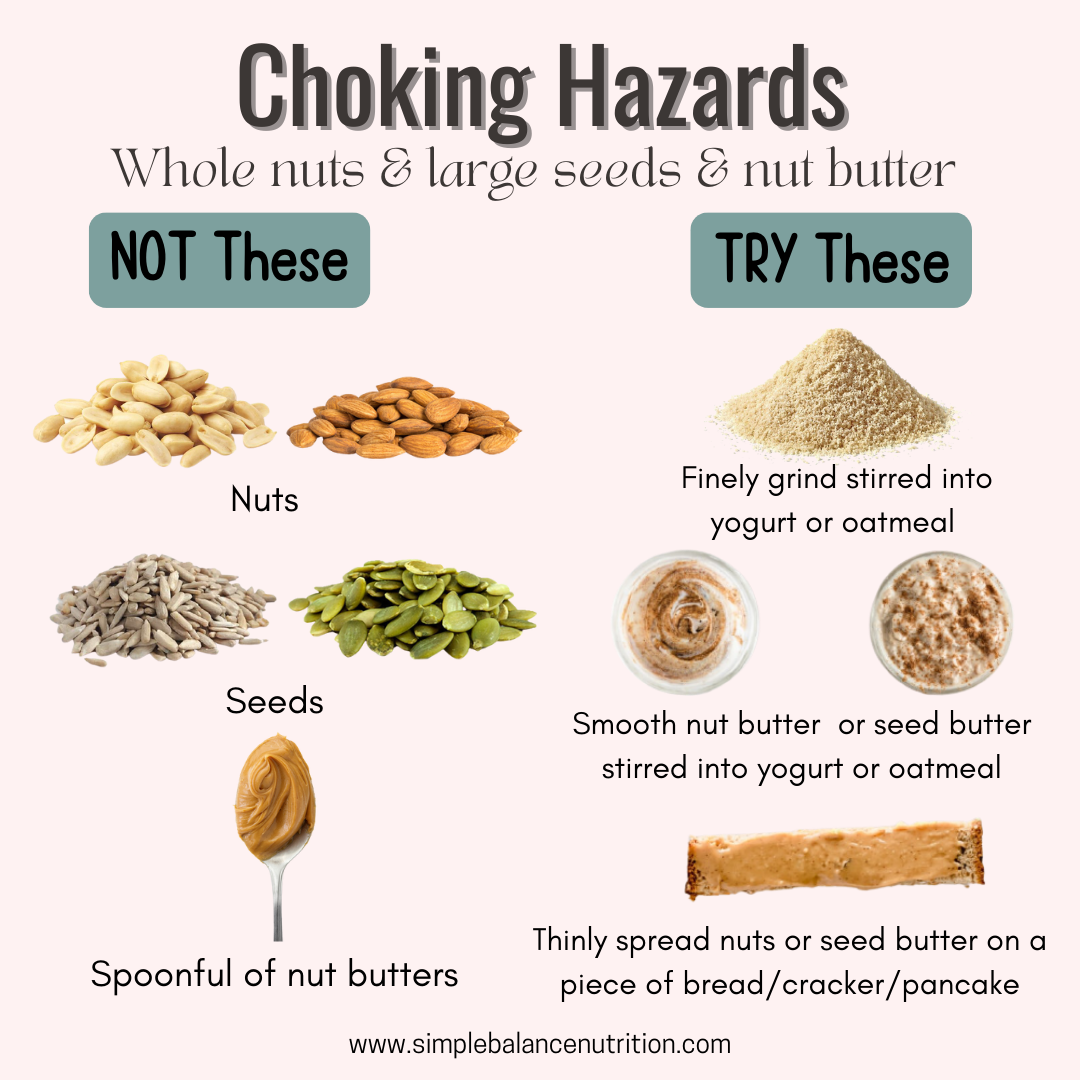
Whole nuts pose a choking hazard and should not be offered to children under the age of 4. Additionally, chunky nut butter with large lumps should be avoided for the same reason. To ensure safety, serve nuts to young children in alternative forms such as puffs, nut powder, finely chopped, in the form of flours, thinned nut butter, or incorporated into purees. These preparations minimize the risk of choking and make nuts more suitable for young children’s consumption.
ARE NUTS A COMMON ALLERGEN?
Peanuts and tree nuts are all classified as top food allergens, so it’s important to be vigilant about any potential reactions when introducing foods containing nut ingredients to your baby. Allergic reactions can occur within minutes to hours after consumption, so it’s advisable to offer such foods at a time when you can closely monitor your child for a few hours, rather than during dinner.
Be attentive to possible symptoms of an allergic reaction, which may include itchy rashes, hives, vomiting, difficulty breathing, swelling of the lips and tongue, and, in severe cases, anaphylaxis. Promptly contact your pediatrician if any of these symptoms occur.
FEEDING TIPS WHEN INTRODUCING NUTS
Nuts pose a choking hazard for babies and young children, so it’s important to avoid offering whole nuts, chunks of nuts, or large dollops of nut butter to ensure their safety.
Serve nuts earlier in the day:When introducing a new type of nut, offer it during breakfast or lunch so you can closely monitor your baby for any potential allergic reactions.
Start with a small amount: You don’t need to give your baby a large serving to check for reactions. Begin with a small quantity to gauge their tolerance.
Never rub on your baby’s skin:This will not help to identify a food allergy and can actually increase the risk of an allergy developing.
Keep it on the menu: After successfully introducing a specific type of nut into your baby’s diet, aim to include it regularly in their weekly meal plan. This consistent exposure can potentially reduce the risk of developing allergies later in life.
HOW TO INTRODUCE PEANUTS OR TREE NUTS TO BABY
Begin by introducing one type of nut early in the day, allowing you to closely monitor for any potential symptoms. To ensure safety and to thoroughly assess for any overlooked reactions, it is recommended to reintroduce the same variety of tree nuts or peanuts the following day, preferably around the same time. To monitor any allergy reactions, it’s best to wait 1-2 days before switching to a different type of nut.
Here are some of my favourite ways to introduce peanuts and tree nuts to your baby’s diet:
FOR TRADITIONAL WEANING
Add a small amount of warm water to a teaspoon of nut butter. Blend until you reach a smooth consistency, never serve a globs of nut butter as it can pose a choking hazard for young children.
Infant cereal or oatmeal: Mix nut butter or finely chopped nuts into baby’s meal for added flavor and nutrition.
Purees: Add a small amount of nut butter or finely chopped nuts to homemade baby purees for added texture and nutrition.
Smoothies: Blend nut butter into a fruit or yogurt smoothie for a creamy, nutty flavor.
FOR BABY LED WEANING OR FINGER FOODS
Pasta tossed with pesto(if making at home, you can change which nuts or seeds you use as the base).
Nut butter thinly spread on toast, pancakes, or waffles strips.
Sprinkle finely chopped nuts on slices of banana, avocado, sweet potato wedges, oatmeal, applesauce, or yogurt.
Mixed finely chopped nuts into the batter of pancakes, waffles, and muffins. Use a small amount of almonds to replace some of the regular flour used in baked goods.
Nut butter yogurt dip.
The above methods offer versatility in introducing nuts to your baby’s diet, allowing you to choose the most appropriate option based on your baby’s age and preferences.
RELIABLE DIAGNOSIS OF FOOD ALLERGY IS IMPORTANT
It is important that allergies are accurately diagnosed and confirmed by a medical doctor. Your child’s doctor may conduct skin prick tests or blood tests to assess allergen-specific IgE levels, which can aid in confirming or ruling out potential allergens. However, it’s important to note that while these tests can establish the presence of an allergy, they do not predict the severity of an allergic reaction in individuals with allergies.
It’s also worth mentioning that some other forms of allergy testing lack scientific evidence and are therefore not recommended.
BOTTOM LINE
Many foods are suitable for young children, but whole nuts are a choking hazard until at least age 4, and spoonfuls of nut butters can be too sticky for little mouths. The good news is that there are numerous delicious ways to serve nuts, providing healthy fats, protein, and essential nutrients. Nuts are rich in vitamins and minerals like Vitamin E and iron, making them a valuable addition to children’s diets for enhanced nutrition. I hope this blogpost can help you safely incorporate nuts into your baby’s diet while minimizing risks and promoting healthy eating habits.
Did you know that I offer personalized one-on-one nutrition counselling for children and families? If this is something you’s like to learn more about, check out my service.
While I’m a fan of Baby-Led Weaning (BLW), the concern about not getting enough iron intake is real, especially since many moms like to offer fruits and veggies as starter foods for their babies. In fact,this is one of the most common mistakes parents make when practising BLW!
Iron deficiency is estimated to be the most common nutritional deficiency worldwide. It can lead to anemia, impaired growth and development, as well as impaired cognitive function, including delayed attention, learning difficulties and social withdrawal. According to Malaysia’s National Health and Morbidity Survey (NHMS) 2022 Maternal and Child Health report, 46.5% of children between 0-5 years old were anemic. Therefore, contrary to the popular saying, “Food before 1 is just for fun,” the truth is that nutrition in the first year matters greatly.
INCREASED NEEDS
By around 6 months of age, your baby’s iron stores, acquired during pregnancy, begin to deplete. This depletion is influenced by factors such as the mother’s iron levels during gestation, whether cord clamping was delayed at birth, and the baby’s gestational age at birth. In fact, about 80% of a baby’s iron stores are built up during the third trimester of pregnancy, which means that bring born “overdue” can sometimes be an advantages in this context.
By six months, however, babies still obtain some iron from their breast milk or formula, but it is no longer enough to meet their growth needs. This is why the introduction of solid foods becomes crucial, not to replace milk, but to complement it. These first foods are often called “complementary foods,” for this reason.
This leads us to the key question: How much extra iron do babies need, and what are the best food sources to ensure they get enough?
HOW MUCH IRON DOES MY BABY NEED?
So, how much iron does a full-term, healthy-weight baby actually need?
In North America, the Recommended Dietary Allowances (RDA) for iron are:
BABIES 0-6 MONTHS: 0.27 mg/day*
BABIES 6-12 MONTHS: 11 mg/day
TODDLERS 1-3 YEARS: 7 mg/day
* This value is classified as an “Adequate Intake” Instead of a “Recommended Daily Allowance”.
In Malaysia, The Recommended Nutrient Intake (RNI) is slightly different:
So, the exact number depends on which guideline you follow. A practical target is about 7-8 mg of iron daily for 6-12 month olds who consume meat, while vegetarian babies, may need closer to 9-11 mg per day.
It’s important to remember that the RDA of 11mg is an average requirement across 7-12 months, which includes both breastmilk/formula and solid foods. Babies’ iron needs don’t suddenly surge overnight at 6 months. Instead, their requirement rises gradually as they grow.
Naturally, there’s a big difference between a 7-month-old just starting solids and a 12 months-old which can eat a variety of foods. The great news is that babies usually adapt quickly, and with BLW, they can progress to eating a substantial amount of food in just a few months.
Most importantly, you don’t need to tract every milligrams of iron your baby eats, doing so can become stressful and unsustainable. Instead, focus on offering a variety of iron-rich foods consistently throughout the day to help your baby meet their needs.
SIGNS OF IRON DEFICIENCY
If you’re worried that your child isn’t getting enough iron, here are some common signs and symptoms of iron deficiency to look out for:
Slow weight gain
Little or no appetite
Pale skin
Fatigue or low energy
Always tired
Cold hands and feet
Brittle nails
Poor immunity (frequent illness or infections)
To help prevent anemia, the American Academy of Pediatrics (AAP) recommends a routine blood test for all 12-month-olds to check iron levels. In Malaysia, if you’ve concerns about your child’s iron intake or notice any of the above signs, it’s advisable to consult a doctor and request a blood test.
If your child’s iron levels are found to be significantly low, iron supplements may be prescribed for a few months. In such cases, diet alone is usually not enough to restore iron levels to normal, and supplementation is necessary under medical supervision.
In the BLISS group, parents were taught to strategies prevent choking, growth faltering, as well as how to ensure an adequate intake of iron-rich foods while self-feeding. They were encouraged to offer at each meal:
A high iron food (e.g., red meat and fortified cereals)
The results showed that 83% of babies in both the control and BLISS groups had adequate iron levels, while anemia was found in 5% of the control group and 7% of the BLISS group. Importantly, there were no significant differences between the two groups in terms of iron levels and stores at either 7 or 12 months of age.
This is promising news! It suggested that with the right education and guidance, BLW can be a nutritious and safe approach to introducing solid foods without increasing the risk of iron deficiency.
So, Can BLW Babies Get Enough Iron?
The short answer is YES! It is absolutely possible.
Traditionally weaned babies often rely on iron-fortified rice cereal as their main source of iron, which is usually skipped in BLW. But, BLW babies can still meet their iron needs. In fact, BLW babies are often introduced to meat earlier if it’s part of the family’s diet, whereas traditionally weaned babies may not eat meat right away at the beginning of starting solids.
Research shows that as long as parents consistently offer iron-rich foods at each meal, there is no significant difference in the iron status between babies following BLW and those fed purees.
For vegetarian and vegan babies, meeting iron needs may be more challenging, but it is achievable with careful planning. Offering a variety of iron-rich plant-based foods, such as legumes, tofu, leafy greens, and fortified cereals, paired with vitamin C-rich foods to boost absorption, can help ensure adequate intake. In some cases, including fortified rice cereal may also be beneficial.
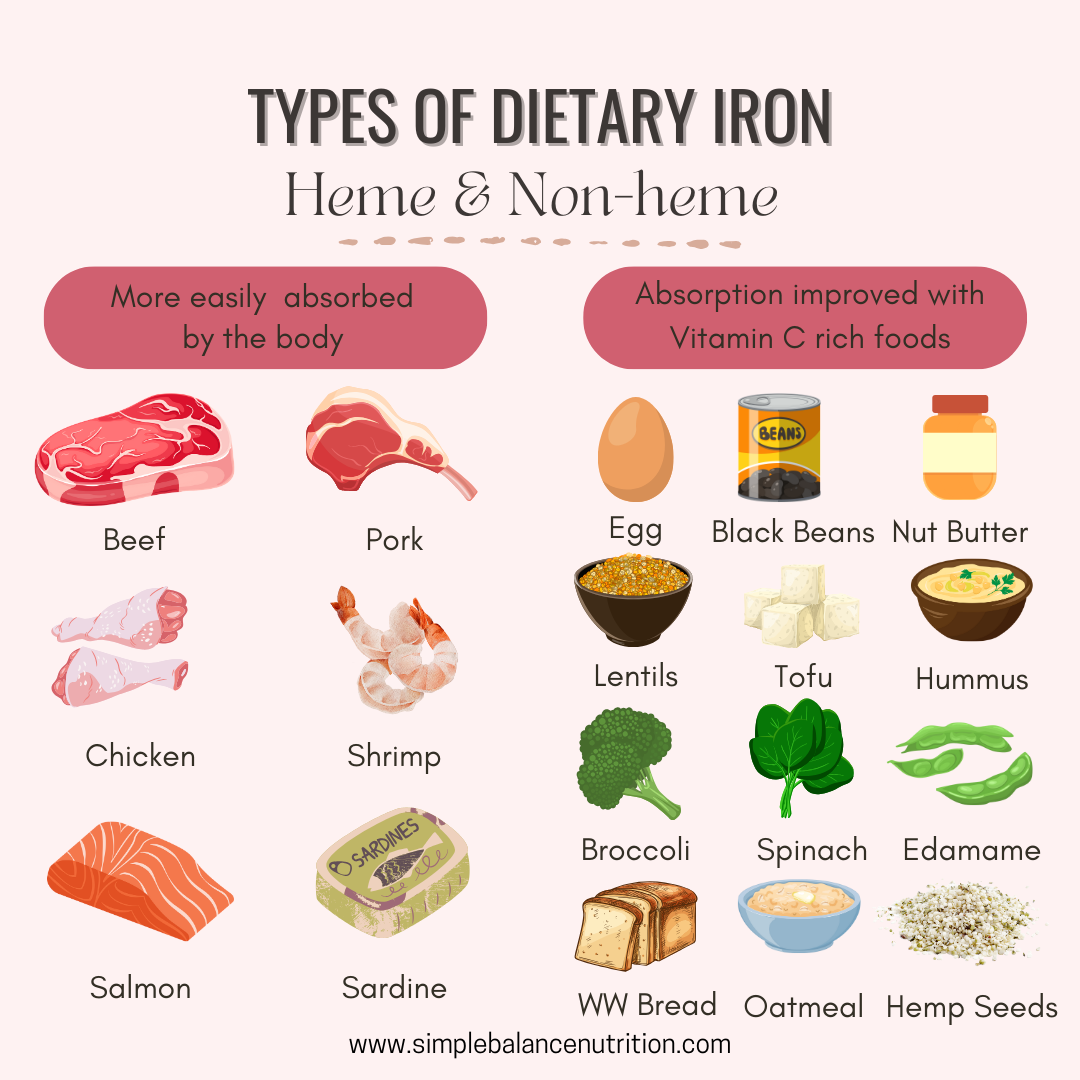
WHAT FOODS ARE HIGH IN IRON
There are two main types of dietary iron: heme and non-heme.
Heme iron, found in animal products like meat, fish, and poultry, the human body has a high absorption rates at approximately 20%.
Non-heme iron, found in plant sources like soy, lentils, beans, and even eggs, but it is less readily absorbed by the body, with only about 10% uptake.
This difference in bioavailability means that not all iron sources are equal.
I don’t believe in focussing too much on numbers or counting exact milligrams of iron every day, as this approach can lead to unnecessary stress. However, I do think it is useful to know the amounts of iron found in realistic serving sizes of some common foods. Here are some examples:
Chicken (75 g) = 0.4-2 mg (dark meat has higher levels than white meat)
Sardines, canned (75 g) = 1.7-2.2 mg
Tuna, light, canned in water (75 g) = 1.2 mg
*While liver is an excellent source of iron, it contains an excessive amount of preformed Vitamin A, which can be toxic for young children. The Upper Limit recommended for ages up to 3 years is 600 micrograms, whereas just 1 oz of liver contains over 5,000 micrograms. Plus, the liver is the filter for our body and may contain trace metals, so it should not be a regular food for babies.
Ways to serve heme-iron foods in BLW:
Ground meat sauce on pasta or rice
Mini baby burgers or meatballs
No-added salt canned sardines as finger food
Pressure or slow-cooked pork or beef roast, shredded
Pork ribs or chicken legs (removed skin, gristle and small bones)
Boneless chicken thighs, cut into finger-sized strips
Sprinkle wheat germ or hemp hearts onto yogurt or blend into a smoothie
Spread hummus on a toast fingers
Offer black beans as finger food for practicing their pincer grasp
Smush larger beans like chickpeas with your finger, to reduce choking risk
Bean or lentil patties
Spread nut butters thinly on toast fingers
TIPS TO GET ENOUGH IRON WHILE USING BLW (6-12 months)
1. Continue offering adequate breast milk or formula as the baby’s main source of nutrients.At this age, solid foods serve as complimentary foods, helping to boost nutrient intake while gradually preparing your baby’s digestive system for the full transition to solids.
2. Ensure that every meal includes a source of iron, both heme and non-heme iron.
3. Incorporate fortified infant cereal baked into baked finger foods for an easy iron boost. You can also replace half of the flour in pancake recipes with fortified infant cereal to increase iron content.
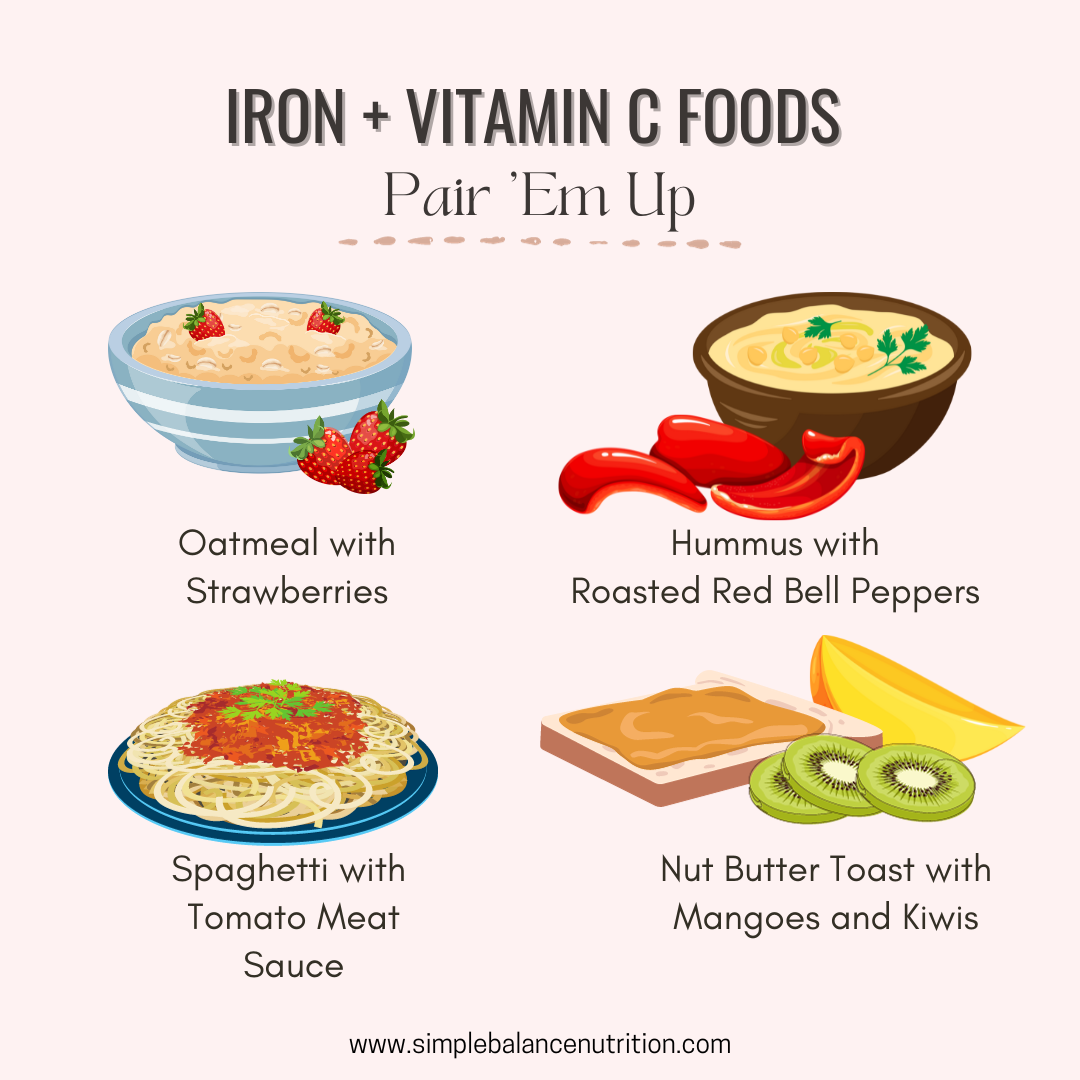
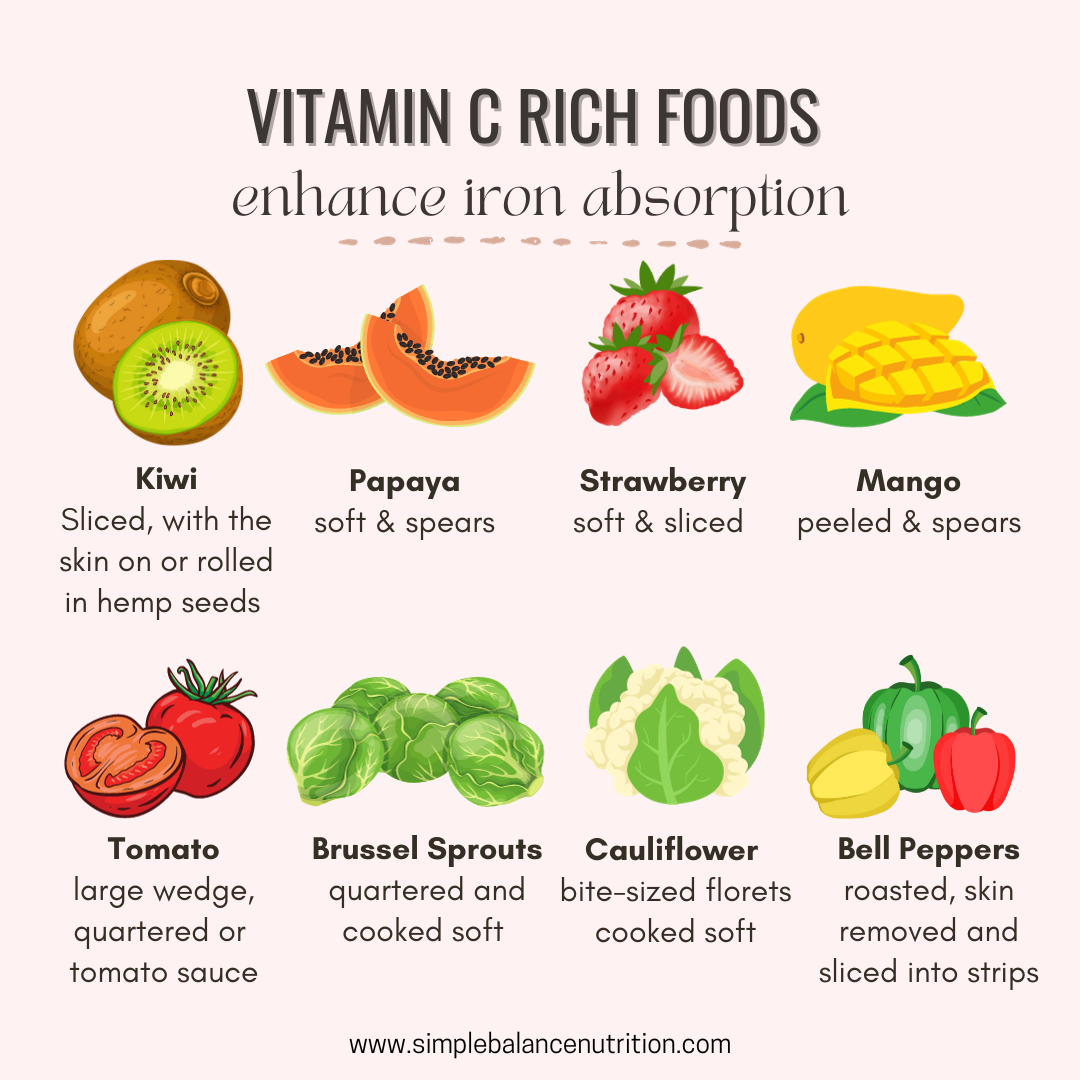
4. Pair iron-rich foods with vitamin C rich foods, to increase the absorption of non-heme iron in the body. For example, top fortified pancakes or cereal with fruit compote; serve lentils in stewed tomatoes and add spinach to a fruit smoothie.
Other excellent sources of vitamin C, including bell peppers, tomatoes, broccoli, citrus fruit and berries, etc. Combing ground meat with a tomato-based sauce creates an ideas meal that provides both heme iron and vitamin C to boost absorption.
5. Cook with cast iron cookware.Cooking with cast-iron pots and pans can safely increase the iron content of your meals. If you don’t have cast-iron cookware, you can try a product called the Lucky Iron Fish®. This simple, reusable and effective cooking tool that adds extra iron to your daily foods, soups or drinks. It is an affordable and effective solution, especially for families managing iron deficiency anemia.
6. Cook with garlic or onion.Preparing meals with allium-containing ingredients, such as garlic and onions can help increase iron absorption.
BOTTOM LINE
Regardless of which feeding approach you choose, it’s important to introduce iron-rich foods around 6 months of age, once your baby shows developmental readiness for solid foods.
Babies following the Baby-Led Weaning approach can absolutely meet their iron needs by offering a variety of iron-rich food at each meal.
Want more tips to make Baby-Led Weaning easier and more enjoyable for your little one? Enroll in our online course, Baby’s First Bites, and get step-by-step guidance to help your baby thrive at mealtimes.
Many parents are terrified of feeding their baby beyond purees or finger foods.
“Is there a risk of my baby choking if I introduce finger food?”
“What is the difference between gagging and choking?”
“How to prevent my child from choking?”
“What should I do if my baby starts choking or gagging?”
“How can I overcome my intense fear of choking when feeding my baby?”
DOES BLW INCREASE THE RISK OF CHOKING? (WHAT THE RESEARCH SAY)
A 2021 review study quoted: “Fear of choking was an important factor in parents’ decision not to implement BLW; however, this fear was not supported by the literature.”
Today, I will provide a breakdown of two studies that have examined the risk of choking associated with Baby Led Weaning as a method for introducing solids.
THE BLISS STUDY
BLISS stands for “Baby-Led Introduction to Starting Solids”. This clinical trial on choking was published in the “Pediatrics” journal and titled “A Baby-led Approach to Eating Solids and Risk of Choking” This study included 206 families.
During the study, parents completed questionnaires at 6, 7, 8, 9, and 12 months of age regarding their baby’s choking and gagging experiences. Additional follow-up questions were asked to parents who reported incidents of choking to gather information about the type of food consumed and how the choking was resolved.
The findings revealed that approximately 35% of babies experienced at least one episode of choking between the ages of 6 and 8 months. There was no significant difference in the incidence of choking between the two groups at any of the assessed time periods.
However, it was observed that babies who started with Baby Led Weaning initially experienced more frequent gagging at 6 months, which decreased by the time they reached 8 months. On the other hand, babies in the puree group exhibited an increase in gagging incidents by 8 months, likely due to their progression to consuming finger foods. It is important to note that the gagging stage is a normal part of learning to eat and cannot be entirely avoided.
Regarding cases where medical assistance was required due to choking, two babies choked on milk, while one choked on food that was placed in their mouth by a caregiver (it is not recommended with Baby Led Weaning). This highlights the fact that choking can occur with any type of food or substance.
Furthermore, the researchers discovered that both groups frequently offered choking hazards to their babies, and not all parents closely supervised their babies during feeding.
In a survey conducted by Dr. Brown, 1151 mothers with babies aged between 4-12 months were interviewed. The mothers provided information on the method used to introduce solids (strict BLW, loose BLW, or traditional weaning) and the percentage of mealtimes involving spoon-feeding purees.
The survey also inquired about instances of choking experienced by the babies, including the frequency and the type of food involved (smooth puree, lumpy puree, or finger food).
The results indicated that 13.6% of the babies (155 out of the 1151) had experienced choking incidents. However, no significant correlation was found between the chosen method of introduction (BLW or traditional) or the frequency of spoon-feeding purees and the occurrence of choking.
It is noteworthy that among the babies who experienced choking, those following a traditional weaning approach had a higher number of choking episodes associated with finger foods and lumpy purees compared to babies following either strict or loose BLW.
This observation raises potential hypotheses: BLW mothers might exhibit lower anxiety levels, leading to less overinterpretation of choking incidents or excessive assistance during feeding, which can pose risks. Alternatively, the higher incidents of choking among traditional weaning babies could be attributed to their lower exposure to finger foods in the early stages, resulting in less practice when the gag reflex is more sensitive. This finding emphasizes the importance of introducing finger foods from the beginning, regardless of whether purees are included in the feeding approach.
Overall, based on the research, it suggests that the potential risk associated with BLW is not significantly higher compared to a traditional approach when initiating solid foods.
IS MIXED FEEDING SAFE?
Both Health Canada and the National Health Services (NHS) in the UK actually recommend a combination approach when introducing solids, which includes offering both finger foods and purees right from the start.
Despite some adamant claims made by Baby-led Weaning Facebook groups suggesting that this method increases the risk of choking, both research findings and personal experiences from my clients and my own child have not supported this belief.
Therefore, if you choose to incorporate both pureed foods and finger foods into your baby’s diet, there is no need to strictly adhere to the label of “Baby-led Weaning.” The important thing is to follow responsive feeding practices when spoon-feeding purees, being attentive to your baby’s hunger and fullness cues to avoid overfeeding. Additionally, make sure to offer finger foods during each meal to provide opportunities for your baby to practice self-feeding.
Ultimately, what matters most is following a feeding approach that suits your baby’s needs and abilities, regardless of the specific labels or guidelines, while prioritizing their safety and nutritional needs.
GAGGING
WHAT IS GAGGING?
Gagging is a natural reflex that helps prevent choking by stopping us from swallowing. It’s a normal and important part of learning to eat solid foods for babies. Gagging brings the food up to chew more before it goes back down, ensuring that only well-chewed food reaches the back of the throat to be swallowed.
Gag reflex effectively keeps larger food pieces near the front of the mouth, only allowing very well-chewed foods to the back to be swallowed.
During the initial stages of introducing solid foods, your baby’s gag reflex is positioned at the front one-third of their tongue. However, as they gain experience and exposure to different solid foods, the reflex gradually shifts further back. Eventually, it settles at the top of the throat, where the gag reflex is typically located in most adults.
WHAT TO DO IF YOUR BABY IS GAGGING
If your baby is gagging, avoid patting their back or attempting to stick your fingers in your baby’s mouth to remove the food, as this could cause the food to move deeper and potentially result in choking. Instead, demonstrate coughing the food up and spitting it out. Remember to stay calm and relaxed, as your reaction can influence your baby’s response to gagging and make the eating experience less enjoyable for them.
Never interfere! Allowing your baby to stay in control and figure it out on his own.
HOW TO PREVENT GAGGING
To help prevent gagging, there isn’t much you can do during your baby’s mealtime. However, you can start preparing them for learning how to eat by bringing them to the table around 5 months of age. Offer them a “hard munchable” item to chew on, such as a rib bone, celery, or a raw carrot. Although they won’t actually consume it, this will make your baby feel included in the family meal and increase their awareness of their mouth and how it functions. It can also strengthen their mouth muscles and potentially reduce a highly sensitive gag reflex.
WHEN TO GET HELP FOR GAGGING
If your baby continues to gag with every bite after a few weeks of introducing solid foods, it may be necessary to seek assistance from an Occupational Therapist or Speech-Language Pathologist.
Occasionally, babies may gag to the point of vomiting, which is also relatively common. To minimize this, try spacing out milk feedings from solids to ensure their stomach is not overly full during mealtime. This can reduce the likelihood of vomiting and prevent significant calorie loss.
If your baby consistently gags and vomits when eating solids exclusively, it might be beneficial to take a break from introducing solids for now. Your baby may not be quite ready, so waiting until they reach six months of age and then trying again could be a good approach.
For babies older than six months, consider offering purees for a week or two before reintroducing finger foods. While babies can still gag on purees, it might be easier for them to manage initially. Remember, it’s important to follow a baby-led approach if it aligns with your preferences and situation.
CHOKING
WHAT IS CHOKING?
Choking occurs when food accidentally enters the airway instead of the esophagus (food pipe).
During choking, a baby will not make much noise or may be completely silent as their air pipe becomes blocked. It is important to remember that loud gagging noises can be a positive sign in such situations.
When a baby is unable to obtain oxygen due to choking, their breathing is compromised, and their lips and face may turn blue.
IS CHOKING NORMAL FOR BABY LED WEANING
Fortunately, choking is significantly less common than gagging.
When reviewing the research, it is worth noting that approximately 13%-35% of babies in these studies were reported to have experienced choking at least once. Personally, I consider myself fortunate as I never had this experience with any of my children.
WHAT TO DO IF BABY CHOKES?
Choking is much more serious than gagging, and requires immediate intervention.
If there is another adult or older child present, quickly shout for their help and instruct them to call ambulance. In the absence of someone else, immediately make the call yourself while initiating infant CPR. Taking an infant first aid course can provide you with the knowledge and skills to handle such situations with confidence, even though the chances of it happening are unlikely.
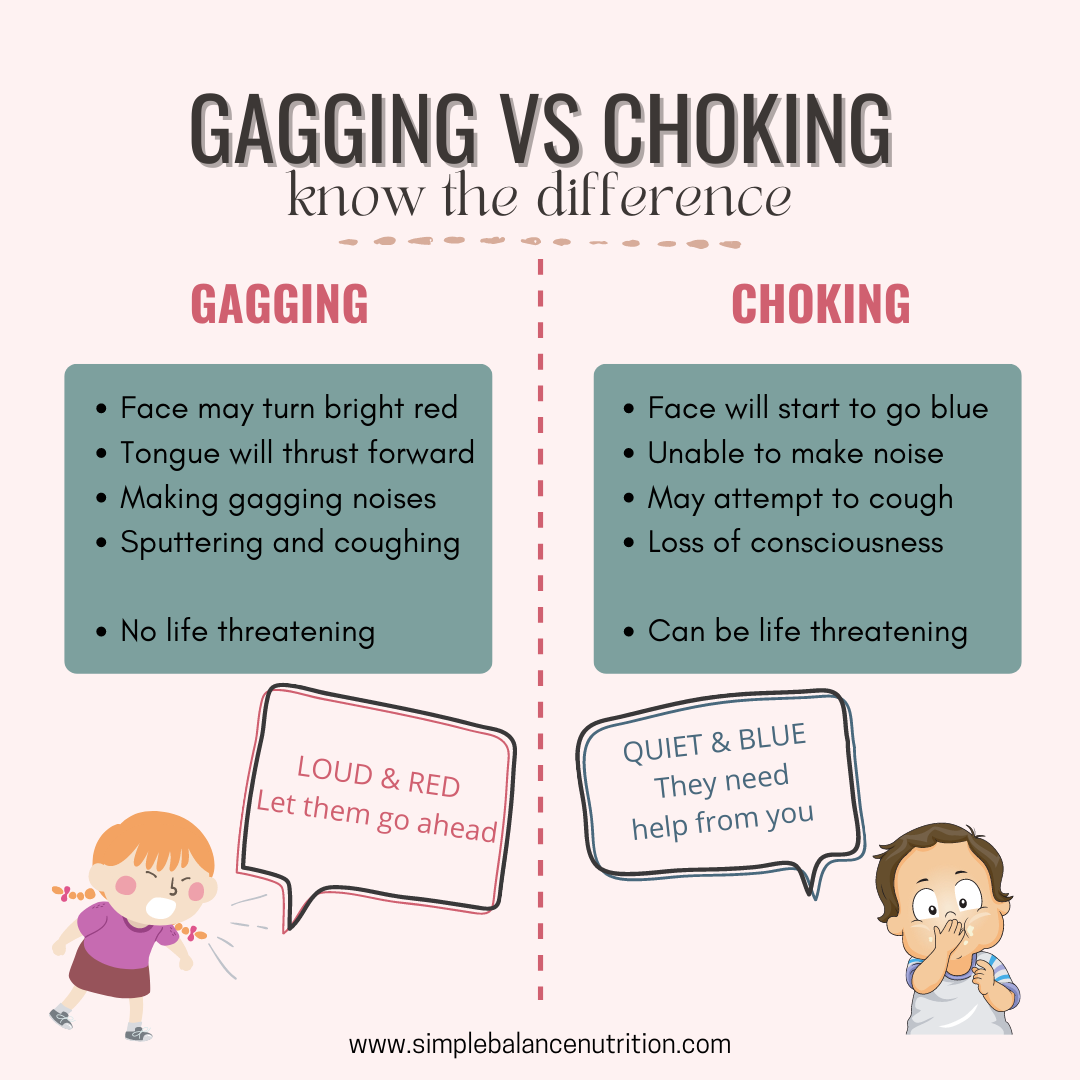
KNOW THE DIFFERENCE BETWEEN CHOKING AND GAGGING
GAGGING
Loud and red = gagging, let baby work it out
Face may turn bright red
Tongue will thrust forward
Making gagging noises
Sputtering coughing
No life threatening
It is advisable to avoid overreacting when your baby experiences gagging during mealtimes, as this may create fear and increase stress for both you and your baby. It is recommended to allow your baby a moment to handle the gag reflex independently without any intervention from you.
CHOKING
Silent and blue = choking, baby needs your help immediately
Face will start to go blue
Unable to make noise
May attempt to cough
Loss of consciousness
Can be life threatening
Choking occurs when food passes beyond the gag reflex and obstructs your baby’s airway, leading to either partial or complete blockage. This can result in a significant reduction or complete cessation of oxygen reaching the lungs, making it difficult for your baby to breathe. Choking is a severe situation that demands IMMEDIATE intervention, and if your baby is choking, it is crucial to promptly initiate infant CPR.
CHOKING HAZARDS
It is important to note that BLW does carry a potential risk of choking compared to offering purees, especially when certain types of foods are introduced. Choking incidents occur when the airway becomes obstructed, which can happen if a baby bites off a piece of hard food that perfectly blocks the air passage. Therefore, careful attention must be given to the size and texture of foods offered during BLW. It is crucial to closely supervise your baby during mealtime and consider taking an infant CPR course as a precautionary measure.
HERE’S A FULL LIST OF POTENTIAL CHOKING HAZARDS
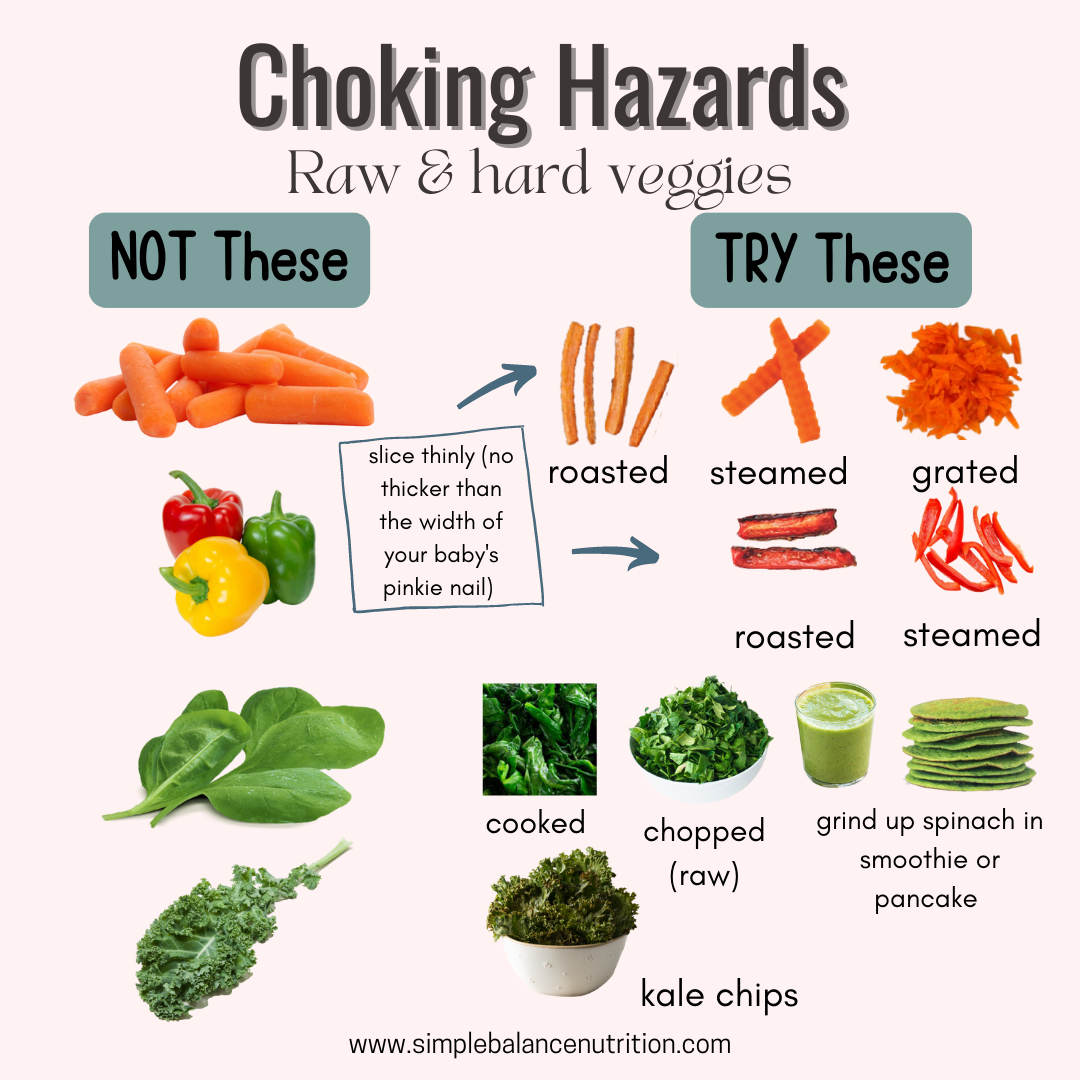
Raw hard vegetables (carrots or beets)
Raw leafy greens
Fibrous and stringy foods (celery, pineapple, or asparagus)
Firm fruit with and without peels (apples)
Fruits with pits or seeds, that haven’t been removed (whole plum or peach)
Whole grapes
Whole blueberries
Whole cherry tomatoes
Dried fruits (raisins, dried apricots)
Chunks of firm meat (steak)
Fish with bones
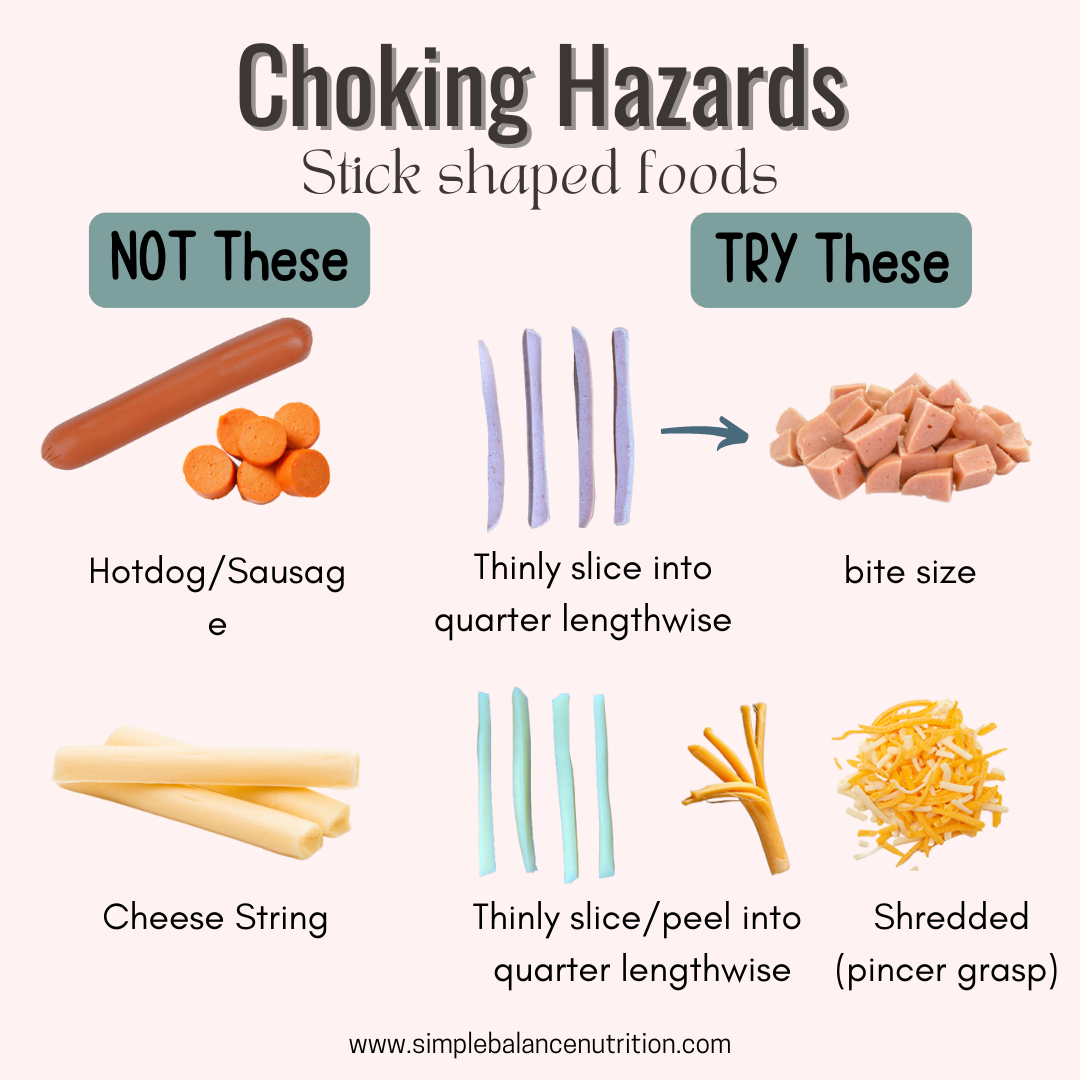
Whole hotdogs or sausages
Cheese sticks
Whole nuts and seeds
Think globs of nut butter
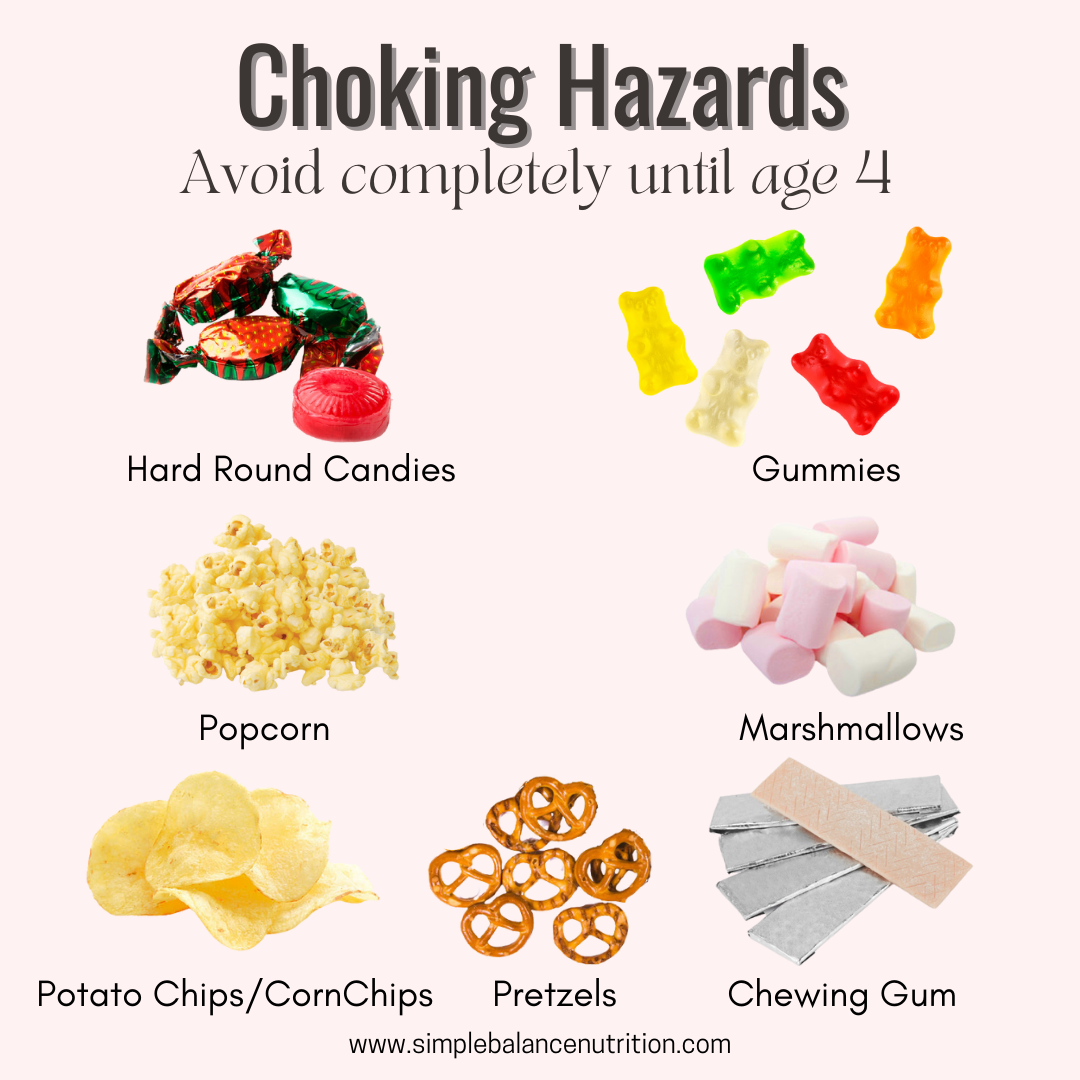
Hard candies, mints, or cough drops
Gummy bears
Popcorn
Marshmallows
Hard chips or nachos
Chewing gum
Snacks with toothpicks or skewers
ALTERNATIVE WAYS OF SERVING:
Steam vegetables and fruit.
Peel and grate hard vegetables and fruit like carrots, apples, and zucchini.
Grate cheese.
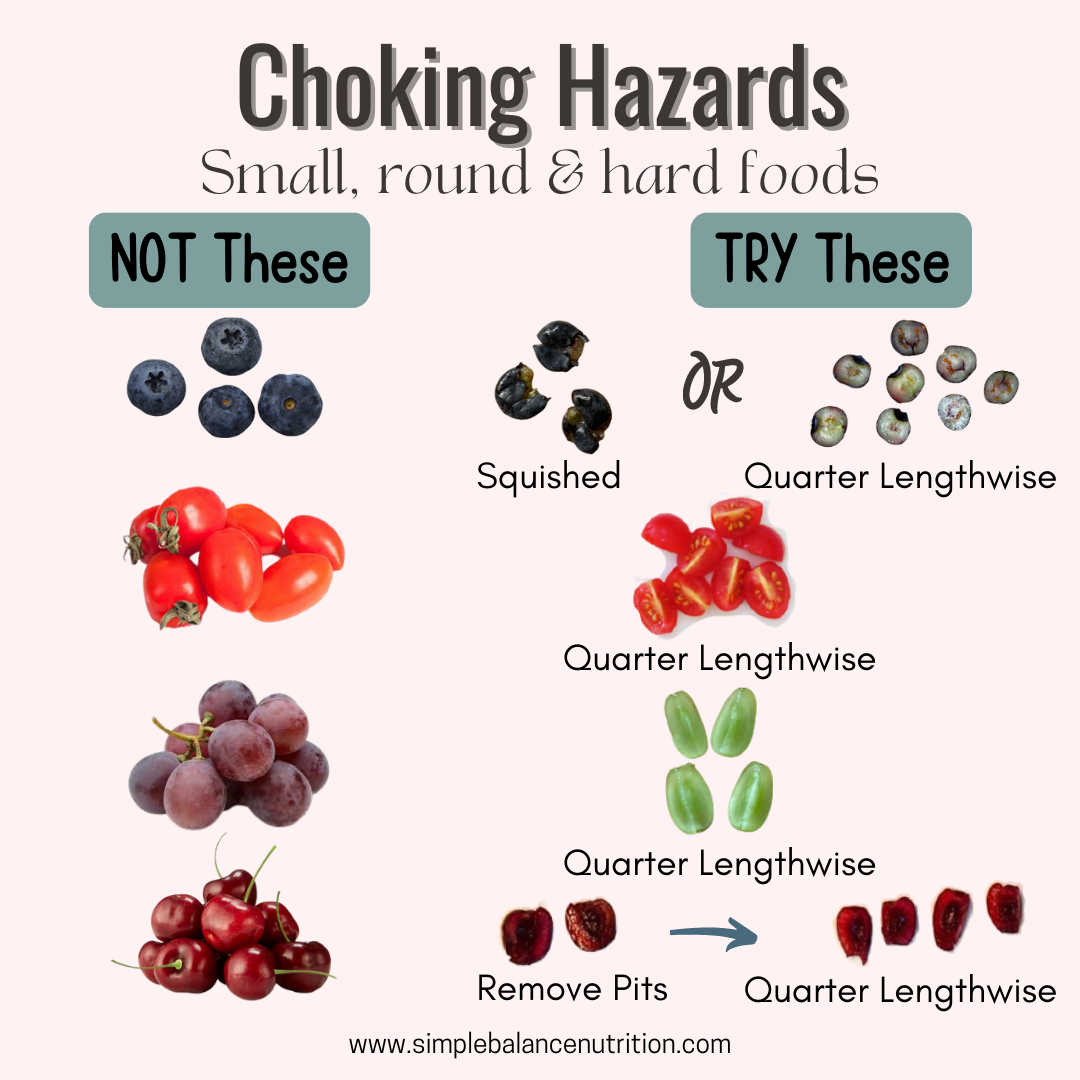
Always remove pits and seeds from fruit.
Slice small and round foods into quarter lengthwise.
Thinly spread any nut or seed butter on toast.
Remove bones from fish or meat.
Serve fresh, frozen, or canned (rinsed) corn instead of popcorn.
Well it’s possible for your baby to choke on food (or toys/coins/may other objects), there is a lot you can do to prevent choking.
TIPS TO PREVENT CHOKING WITH BLW
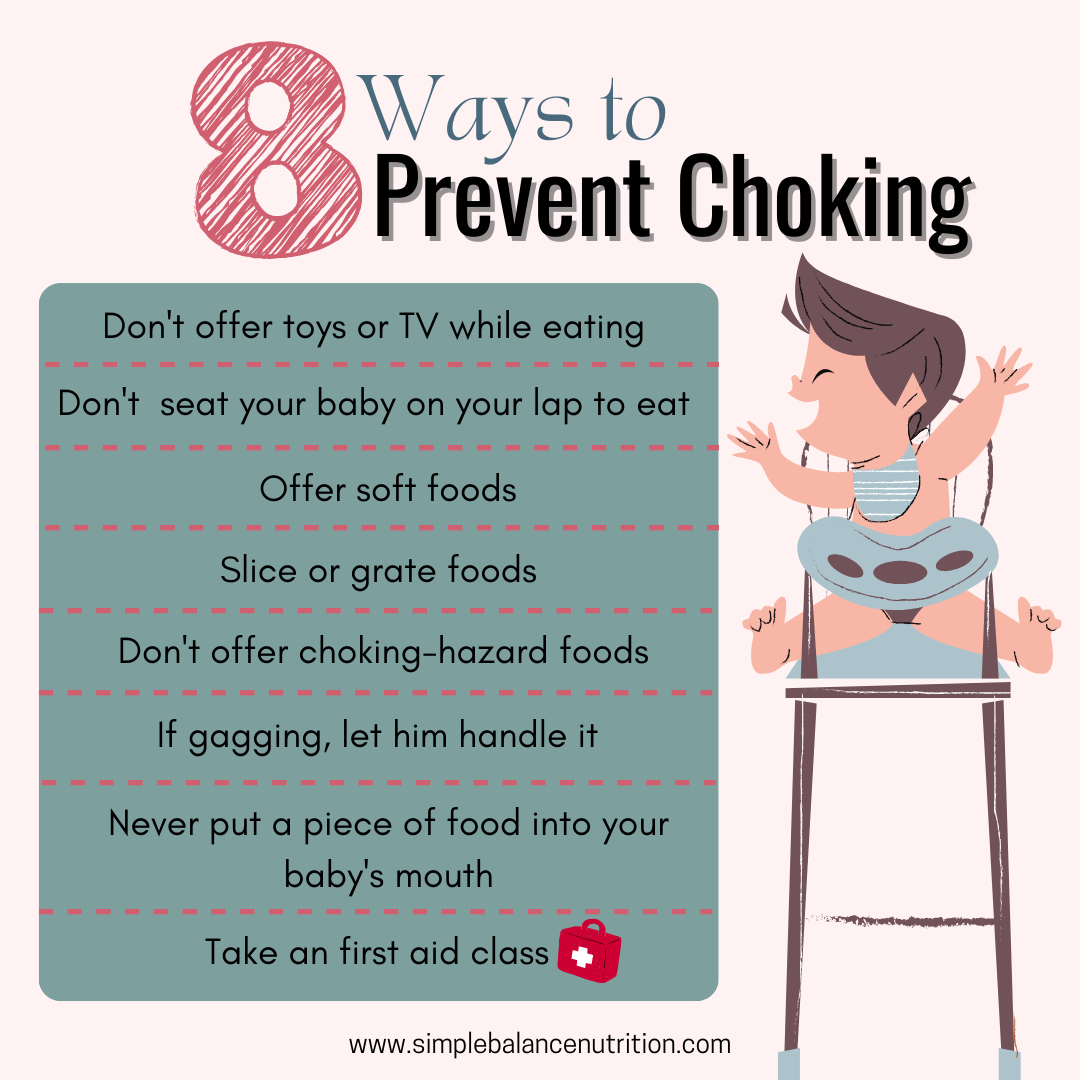
Ensure that your baby is developmentally ready for solids.
Positioning:Make sure your baby is sitting upright during mealtime and avoid a reclining position. Provide proper support by using a high chair that keeps your baby well-supported. Using rolled-up towels if needed to ensure proper positioning, with the tray (or table) positioned between their nipples and belly button.
Minimize distractions: Avoid having toys or the TV on during meals as it may distract your baby and increase the risk of choking. Also, discourage running around with food once baby starts walking.
Supervise mealtime: Always watch your baby while they eat and avoid sitting them on your lap during meals. It is important to have a clear view of your baby’s face while they are eating to ensure their safety.
Let them self-feed: Never put a piece of food into your baby’s mouth. If you put food into their mouth, it may immediately fall to the back, without baby having a chance to control it with their tounge and chew it. Let them feed themselves. Also, never attempt to fish food out of their mouth.
Offer safe size of food:Avoid round items like raw hard pieces of vegetables and fruit. Instead, either grate them or slice them thinly. Whole grapes, blueberries, or cherry tomatoes should also be sliced lengthwise into quarters, so they are not a round shape.
Offer soft foods:Test the foods to make sure you can mash them with gentle pressure from your thumb and forefinger. This is called the “squish test“. If the food is harder, make sure it’s in a safe shape (ex: grated or sliced thinly)
Take an infant CPR course.
BOTTOM LINE
It’s very important for parents to recognise the difference between gagging and choking and the different ways each scenario should be treated.
Remember that gagging is a normal reaction that weaning babies have as their gag reflex is triggered while learning to eat. Choking is when their airway gets blocked, and requires immediate first aid and medical attention.
Hope this was helpful. Please check out more about food textures, finger foods and choking on my IG highlights.
Did you know that we offer personalized nutrition counselling for kids and families? If this is something you’d like to learn more about, please visit here.
HIt seems like everyone is sick recently. COVID-19 is still circulating like crazy, but children are also getting hit with Respiratory Syncytial Virus (RSV), strep throat, stomach bugs, HFMD, the flu and other seasonal viruses. As disruptive as illness can be for work, school, and your family’s plans, it can also impact how you and your child eat. How can we feed our children who are sick so they’ll get better faster?
LOWER YOUR EXPECTATIONS
In most cases, when children are sick, it is very normal to see them have very little appetite, no interest in eating, and may even refuse food they usually eat. Even as adults, when we’re not feeling well, we tend to prefer bland, plain foods that are easy to eat as well our favourite comfort meals. We don’t usually fancy a huge variety of exciting foods when we’re not feeling well.
However, it doesn’t mean that you have to ONLY offer bland or favourite snacks to your children. The best thing to do during sick days is to keep your normal feeding routine as much as possible and rely on your child’s internal body signals. Because it’s important to help them keep their energy up and prevent pickiness after illness, and we know it’s usually only for a short period of time and it’s not going to undo any of the work that you’ve done in encouraging them to enjoy a variety of foods.
Responding to their appetite
You can continue to serve other foods alongside to keep up the variety that they are actually familiar with, but don’t be surprised if they’re not touched, or even expect them to try new foods, or foods that they’re less keen on at this time. Their appetites are likely to be all over the place, it can be hard to predict. Therefore, offering foods at set schedule whether they ask for it or not, and trust their body instincts to do the rest in terms of whether food is accepted or how much is accepted.
If they ask for food outside of mealtimes or seem hungry, that’s perfectly fine to give it to them, especially if you’re finding that there have been a few days where not much at all has been eaten. So let them follow their appetite and give them the chance to eat if they show interest. REMEMBER, it’s ok for the routine to slip as it is only for a short period of time. However, once they start to feel a little better, it’s helpful to start to build in some more structure to get things back on track.
FEED YOUR CHILDREN WHEN THEY’RE SICK WITH
i) a cold and respiratory illness
When your child has a cold or respiratory illness, it may affect their appetite and drive to eat. Between coughing, fatigue, a runny nose and sore throat, they might not want to eat or drink like they usually do. They might be tired or uncomfortable, or maybe they’re unable to smell or taste food appropriately.
The biggest concern during illness is keep the body well-hydrated to prevent dehydration. While a child might not eat as much as usual, as long as they’re drinking adequately they should be okay in the short-term.
Babies:
For babies under 12 months, getting enough milk to stay hydrated is most important during illness. Babies will likely prefer sticking to breastmilk or formula, and that’s OK. If your baby has really bad congestion, the use of a bulb suction or Nasal Spray to clear up the congestion might make eating and drinking easier. Focus on regular breastfeeds or bottle feeds and watch for 5-6+ wet diapers per day. If your baby is eating solids (6+ months), offer solid meals like usual but don’t be surprised if your baby isn’t interested. Stay consistent and continue to include your baby in family meals, as long as they’re not upset when they sit in their high chair.
Toddlers ++:
Continue to offer the regular food/meals you normally would at regular times but trust their hunger and fullness cues. Focus on lots of veggies, fruits, protein foods, whole grains and fats. Do not force or pressure them to eat. Nutrition is important during illness, but their appetite and food preferences almost definitely change. You may find your child gravitating toward certain foods or surviving on familiar beige foods like bread and crackers – this is OK. You might want to just feed them whatever sounds good for a while until they feel better. As best you can, try to offer some variety in the food groups you serve, too. They might surprise you when they are suddenly interested in something again.
Sometimes it helps to integrate warm foods into their diet, like clear soup, porridge, mee sua soup or oatmeal. The steam from these foods can help loosen mucus and provide relief from nasal congestion.
The pain of a sore throat can make swallowing food and liquids uncomfortable, which may make your toddler eat less even if they feel hungry. Acidic foods can irritate an already inflamed sore throat.
Avoid acidic foods until your toddler’s sore throat has healed:
orange and orange juice
pineapple juice
tomato soup
Offering extra-cold and smooth foods may help soothe a sore throat:
smoothies blended with frozen fruits
frozen yogurt barks,
popsicles
frozen fruits
Since many cough suppressant medications are not approved for use in young children, it’s hard to know what to do with the coughing child, especially for those night time coughing. Some evidences (here, here, here, here, here) suggest that a spoonful of 100% pure honey can work as a good cough remedy for children over the age of one.
(ii) hand, foot and mouth disease
Hand, foot and mouth disease can be particularly difficult for children and mealtimes. Their mouths can get SO sore, which obviously makes it uncomfortable for them to eat. It’s especially tough as they may actually WANT to eat, they just can’t because it makes the pain so much worse.
Foods for children with hand, foot and mouth disease:
SOFT foods such as yogurt, porridge, cereal or oatmeal are likely to go down well as they are easy to eat and shouldn’t cause too much pain to sore mouths
Scrambled eggs, muffins or pancakes
Soft toast fingers with toppings like avocado, cream cheese, butter or nut butter
AVOID acidic foods such as tomato, citrus fruits or fruit juice
(iii) stomach flu (diarrhea/vomiting)
Stomach bugs or acute gastroenteritis will almost certainly affect the amount and types of food your children eats.
Babies:
Just like with respiratory illnesses, hydration is most important when babies are sick with GI bugs. Dehydration is especially dangerous with stomach bugs because babies can quickly lose fluids from vomiting and diarrhea. Continue to offer regular breastfeeds and bottle feeds and watch for 5-6+ wet diapers per day. If your baby is continually vomiting or has profuse diarrhea and you’re worried about their hydration status, speak with your doctor right away. Make sure your baby can tolerate breast milk or formula before offering bland foods like banana or crackers, then offer a regular diet if bland foods are tolerated.
Toddlers++:
Some simple guidelines to remember when our children are vomiting or have diarrhea:
Start with small amounts of liquids to prevent dehydration.
If those are tolerated, move onto a bland foods like toast, soup/broth, porridge, crackers, oatmeal, eggs (steam) or certain fruits (applesauce, banana, avocado, berries).
Once bland foods are tolerated, move onto a regular, varied diet including complex carbohydrates, lean meats, dairy, fruits and vegetables. Just avoid super heavy and greasy foods like fried or fried chicken, pizzas. The BRAT (banana, rice, applesauce, toast) diet is no longer recommended by the American Academy of Pediatrics. The reason is this diet is low in calories, protein, fat, fiber and other nutrients, also it makes diarrhea last longer. Current research show that children who eat a balanced diet recover quicker from stomach flu.
Juice is generally not recommended during stomach flu because it contains a lot of fructose and sorbitol, which can actually worsen diarrhea. If juice is all your children will drink, make sure to dilute it.
Sometimes water isn’t sufficient to rehydrate children when they’re losing fluid quickly from profuse vomiting or diarrhea. Oral Rehydration Therapy (ORT), means to drink solutions that are made with an appropriate amount of salt, sugar and fluid to help your child’s body absorb lost electrolytes appropriately. Sugar is essential in Oral Rehydration Solutions (ORS) because it helps to get the electrolytes through the bloodstream quicker and to rehydrate your children faster.
Some families make their own inexpensive ORT at home using the World Health Organization recipe. It is just as effective as expensive rehydration drinks and doesn’t contain any harmful ingredients and no dyes.
1/2 tsp salt
6 tsp sugar
1L water
HYDRATION IS REALLY IMPORTANT WHEN CHILDREN ARE SICK!!!
During periods of illness, the number one concern is DEHYDRATION.
Babies:
Under 12 months, babies should still be consuming at least 20-24 ounces of breast milk or formula.
Toddlers ++:
Toddlers and older children need to drink lots of water to stay hydrated and get better. Estimated fluid needs per the American Academy of Pediatrics are as follows:
1-3 years: 4 cups (32 ounces or ~1 L)
4-8 years: 5 cups (40 ounces or ~1.2 L)
9-13 years: 7-8 cups (56-64 ounces or ~1.7-1.9 L)
Fever, diarrhea, vomiting, or just refusing liquids for a prolonged period of time can put your toddler at serious risk for dehydration.
How to prevent dehydration
The best way to prevent dehydration and replace fluids lost through vomit, diarrhea, or sweat is to keep a cup full and encourage your child to sip from it all day long. Using a favorite cup, or straw cup to spark a toddler’s interest in drinking more.
Water is the best choice, of course, but if you’re finding it a struggle to get your child to drink it, here are some other drink ideas:
Water or infused water
Honey lemon water (except children under the age of 1 can’t have honey due to the risk of botulism)
Breastmilk
Fresh cow’s milk/plain kefir
Plant-based milk (ex: soy, almond, oat)
Popsicles or freezies
Smoothies (If your child can tolerate some heavier textures, then a smoothie is a great way to boost nutrition along with fluids)
Bone broth (homemade bone broth has the benefit of protein and additional vitamins and minerals)
Coconut water (diluted 1:1 ratio with water) (offered occasionally, it can be a good substitute if your child likes the flavor, but it’s much lower in potassium than ORT and may not rehydrate as effectively).
Fruit juice (diluted 1:1 ratio with water) (offered occasionally, DON’T offer if experiencing diarrhea. The risk of dehydration FAR outweighs the risk of added sugars in a juice box)
Non-caffeinated tea in small amounts (¼ cup offered occasionally) like Chrysanthemum tea, barley tea, Luohanguo tea 罗汉果
In addition to offering more beverages, if they can still eat, make sure to offer lots of Hydrating Foods (foods with high water content) throughout the day.
Instead of worrying about how much they are actually drinking, watch your child. Make sure they’re urinating regularly and don’t show signs of dehydration.
WHAT ARE THE SIGNS OF DEHYDRATION
Dehydration can be dangerous for a child and severe cases may require hospitalization. If you suspect your child might be showing signs of dehydration, it’s best to call your doctor right away so they can guide you on what’s best to do. According to the American Academy of Pediatrics, the following are signs of dehydration:
Mild to moderate dehydration:
Less activity than usual
Less than six wet diapers a day
Less saliva or cracked lips
Fewer tears when crying
Sunken soft spot on the head
Severe dehydration (all the symptoms listed above, plus):
Very fussy or overly sleepy
Sunken eyes
Cool, discolored hands and feet
Wrinkled skin
Only 1 or 2 wet diapers in 24 hours
Dry tongue and mouth
No tears when crying
GAIN BACK APPETITE AFTER ILLNESS
Appetite after Illness
Ever notice that it takes a few days to even weeks for your children’s appetite to return after they have been sick? Try not to panic that they’ll never eat a variety again. During illness, this is not a good time to force them to eat anything or to buy them French fries, just to get them to eat.
Another thing to remember is after an illness, your child’s taste buds may be dampened. Viruses can inhibit taste and smell function, and sometimes congestion prevents them from smelling (and thus tasting) appropriately. You may experience this as an adult, too. Adding highly flavorful food to their regular meals can help “wake up” their tastebuds and get them back to eating like normal again!
One strategy I love to use is to offer a highly flavorful, crunchy, sour or salty food once or twice a day to help “wake up” their taste buds. I found that children who have been sick sometimes seek out these flavors so they can taste again. Try foods like:
Freeze-dried fruit (mango, strawberries, raspberries)
Cucumber or tomato paired with a strongly flavored dip like hummus or guacamole
Olives (remember to remove pits and quarter lengthwise for kiddos under 4 years old)
Ground meat seasoned with cumin and garlic
Cooking with flavorful spices like cinnamon, ginger and paprika
You can also try lemon, lime or spicy food (if your children usually enjoys and tolerates it).
Don’t be surprised if your child’s appetite takes a while to return to normal when they have been sick. If they seem to be losing weight or not improving over time, consult a dietitian.
DOES VITAMIN C HELP WITH ILLNESS?
There may be NO STRONG evidence to suggest vitamin C will cure a cold. While some studies have suggested that vitamin C may shorten the duration of illness, other research does not support this theory. Plus, giving your children high vitamin C doses can cause diarrhea and stomach upset.
According to the NIH, here are vitamin C needs based on age (daily):
7-12 months: 50 mg (Adequate Intake)
1-3 year-olds: 15 mg
4-8 year-olds: 25 mg
9-13 year-olds: 45 mg
In general, unless your child has an extremely limited diet or malabsorption issues, they likely don’t need a vitamin C supplement.
FOODS HIGH IN VITAMIN C
Since vitamin C can’t cure a cold, but it can support the immune system. Oranges are not the only way to get your daily dose of vitamin C! Many fruits and veggies – yes, even bell pepper – can fulfill a great percentage of your child’s daily needs. Below are some kid-favorite foods that are high in vitamin C:
Potato (medium, cooked) – 15 mg
Tomato (medium, raw) – 16 mg
Mango (1 cup) – 45 mg
Broccoli (1/2 cup) – 61 mg
Orange (medium) – 70 mg
Kiwi (medium)– 75 mg
Strawberry (1cup) – 95 mg
Red bell pepper (1 whole, raw) – 312 mg
Breast milk and formula are great sources of vitamin C, too! In fact, babies’ vitamin C needs are met by their milk alone.
Interestingly, vitamin C also helps our bodies absorb iron, so pairing a high vitamin C food with high iron foods like meats, poultry, fish, lentils, beans and nut butters can help your child’s body absorb iron, a critical nutrient in childhood.
SHOULD MY SICK CHILD AVOID MILK AND DAIRY?
There have been many studies that have looked at the relationship between drinking milk and how it affects mucus production but there is NOscientific evidence to suggest that there is any relationship. However, if you notice your child’s symptoms seem to worsen after a cup of milk or yogurt, you can go ahead and remove it from their diet until they are healthy again.
If your toddler is having a stomach flu, serving dairy can be iffy. It is because sensitive stomach may have a hard time digesting dairy. Again, if you notice any changes or are worried dairy could potentially worsen their symptoms, it’s best to skip it for couple days.
HOW TO GET YOUR CHILDREN TO TAKE MEDICINE?
There’s nothing worse than a sick child who would feel much better if they just took their medicine. If your children refuses prescribed meds, here is an amazing blog post from physician Steve Silvestro, MD on various ways to make taking meds a little easier on everyone.
BOTTOM LINE
Caring for sick children is hard! Be sure to reach out for help and call on your support network for meals or runs to the pharmacy when needed! I hope this article helped to answer your question. For more support feeding children, be sure to check out my 3 months TRANSFORM program.
Note: This information does not replace medical advice. If you have any concerns about your little one’s symptoms, appetite or growth, please do speak to a pediatrician and follow their advice.
Sensory food play is an extremely hands-on activity, which lets children engage with their senses through the exploration of different foods and textures through play. When sensory play is focused on food, it becomes even more stimulating a b se food is the ultimate sensory experience.
I know FOOD PLAY is usually not considered a good thing by parents as it is messy, but it is important for them to explore the foods through play.
Sensory food play is not just about playing foods
WHY?
In a study published in Public Health Nutrition,researchers from Finland describe “sensory-based food education” programs that are common in preschools there. The programs include activities like preparing salads, growing vegetables in a garden or on a windowsill, taking field trips to pick berries, and participating in “sensory sessions” where children touch, listen, taste, and smell different kinds of foods—then share observations with each other.
They found that preschoolers who participated in this food education chose more fruits and vegetables from a buffet compared to those who didn’t receive it. Researchers say this sensory-based education helps children explore food with all five senses and instills a joy of eating. They also note that the findings held true even if there was a high level of pickiness in the group—which shows that “positive peer modeling” can also encourage children to try new foods.
Explore: When we let children explore and play with food, it gives them an opportunity to get to know their food and become comfortable with how it will eventually feel in their mouths.
Stress-free: Some children are anxious about unfamiliar foods, and Sensory Food Play provides them with some much-needed relaxation when faced with the overwhelming sensory experience of a new food. Smashing, squishing, poking, rolling, pouring, and dumping the food can provide stress relief as well as teach them how that food might feel in their mouth (and they just might try it!).
Build Trust: The use of Sensory Food Play can assist the child with touching, smelling and playing with the texture in an environment with little expectation. As the child develops trust and understanding of this texture it helps build positive pathways in the brain to say it is safe to engage with this food.
SENSORY FOOD PLAY RULES:
You can set a time and place for playing with food. You can also set the rules and boundaries for this exploration process. If you are worried about the mess or expense, make a rule about that.
Mess: You can help your children manage their mess with consistent directions and rules. Before you get started, make sure that you have decided where your children are going to be playing. If it is going to be on the floor, put down a splash mat, old shower curtain or blanket. You could also play in the car porch to avoid lots of mess (handy for a rinse over afterwards!). I love to put the infant (6 months+, support with cushion) in highchair and put the messy/food play activity on highchair table. Just remember, the goal is for your children to develop positive feelings and connections with their food, so let them have a little fun with it.
Clean up: Have a clean up bin ready, such as baby wipes, apron, sponge, paper towels, cleaning spray.
Expense: Most of my sensory food play items I buy in bulk (e.g., rice, pasta, beans, cereal, oatmeal, yogurt, food coloring, toothpicks, etc.), which saves money in the long run. I often buy canned food items (peas, pears, fruit cups, etc.) or use leftovers. Also, I use items I receive for free at fast food restaurants (ketchup packets, straws, and other dipping containers).
Sensory food play is so important and beneficial for babies and younger children. Not only is it lots of fun, but there is a lot of learning going on when they are playing that you might not realise. I am going to should you some benefits when a child engages in sensory food play.
SENSORY FOOD PLAY SKILLS:
Sensory system (learning and developing new tastes, textures and smells)
Gross motor skills (body balancing)
Fine motor skills (scooping, pincer grasp, writing, dipping)
Mealtime skills (pouring, tasting)
Language skills (maths, food vocabulary , following directions)
Play skills (imaginary play, solitary play)
Social skills (turn taking, manners) with other children
Problem solving skills (How to..)
Brain development (enhancing memory, ability to complete more complex learning tasks)
Learning cause and effect (what happen after squishing blueberries)
Growing independence through play
Creativity and FUN
Exploring shapes and colours
Here are some fantastic ideas and activities for sensory food play:
Digging in Beans – Get ready to dig, lift, dump, and pour. Fill a pan with dried beans, noodles, or rice and get little trucks or cars out. My son was crazy about this one.
Yogurt Paint – Paint with yogurt. Get your little one touch new veggies while making beautiful art.
Shape Matching – Simple, quick and easy.
Learning Letters – use yogurt to make a letter, and trace the letter with berries or pomegranates.
Stacking – make a tower or building.
Rainbow Toast – Painting on food you can eat!
Counting Game – an easy educational game you can create for your little one.
Food Ribbons – use a peeler to turn a fruit or vegetable into ribbons.
I recommend Sensory Food Play at least once a week at home for picky eaters or problem eaters. Playing with food away from table (without pressure to eat or eat it now) offers your child the opportunity to look at, touch, smell and hopefully tasting the foods.
Sensory food play is vital for a child’s development and learning process! After you discover the key benefits of sensory food play for children in my article today, you may want to initiate sensory food play at home.
DON’T KNOW HOW
If you have no idea, you can check out this SENSORY FUN FOOD PLAY GUIDE. This guide takes you step by step through how to set up food play at home and get your children engaged in more than 100 sensory food play activities. Don’t be afraid to be silly and creative!
As parents, many of us are mindful of how much sugar we give to our little ones, but what about their salt intake, especially if you’re following mixed feeding approach.
HOW MUCH SALT IS TOO MUCH?
Due to limited data for babies, an AI (Adequate Intake) for sodium has been established.
For infants 6 months and younger, the AI for sodium is 110 milligrams per day (here).
For babies between 7 and 12 months old, the AI increases to 370 milligrams per day (here).
This means that for babies under 12 months, the recommended sodium intake is less than 400 mg per day, which includes sodium from both breastmilk/formula and solid foods. Considering that breastmilk and formula contain around 200 mg of sodium per 24 oz., babies should only be consuming about 200 mg of sodium through solid food daily.
The reason for this recommended intake level is that we assume that babies’ kidneys are still very immature and may not be able to process large amounts of salt properly. While there isn’t enough research to definitively say that 400 mg is the maximum safe level for babies under 1 year old, it’s best to stick to this limit until more data is available. Exceeding this could potentially increase the risk of health issues, so erring on the side of caution is recommended.
SALT VS. SODIUM
Salt and sodium are often used interchangeably, and you may see both terms on food labels. However, table salt is actually composed of 40% sodium and 60% chloride.
1 teaspoon of salt = 2300 mg sodium
1 gram of sodium = 2.5 grams of salt
Both sodium and chloride are essential electrolytes (along with potassium) and play vital roles in the body. They help transmit nerve signals, enable muscles contractions, regulate fluids balance, enhance nutrient absorption, maintain acid-base balance, support potassium absorption, and control stomach bacteria levels.
SALT IN FOODS
Salt is found in almost all store-bought, processed, or packaged foods. It acts as a preservative and enhances flavor, so food manufactures often add it deliberately. Common foods that contain salt include:
Processed meats like deli meats, bacon, hotdogs, ham, and sausages
Frozen foods like fish sticks, chicken nuggets, and frozen meals.
Potato chips
Crackers
Canned soups
Gravy
Broths (vegetables, chicken, beef)
Olives, pickles, pickled vegetables (Kimchi)
Soy sauce
Other foods that are high in sodium, even though they may not taste very salty, include:
Cheese and other dairy products like yogurt and milk
Bread, bagels, English muffins, tortillas, and other bread products
Canned tomato and pasta sauce
Canned vegetables
Canned beans
Boxed cereal
*Fresh Milk contains about 100 mg sodium per cup. This is one reason why milk is not recommended as the main drink for babies under one year old. However, a small amount of milk in cereal or baked goods is fine, so there’s no need to eliminate it completely.
WHAT SHOULD YOU DO?
As shown in the picture above, sodium is naturally present in many foods and is often added to processed foods. It’s found in nearly everything we eat. So do you need to completely eliminate salt from your baby’s solid foods?
AT HOME
When cooking meals for your family, you can hold off on adding salt until after you’ve taken out your baby’s portion. For example, when if you’re making a stir-fry, take out a small portion for your baby before adding soy sauce to the rest of the dish.
It’s important not to add salt to anything you prepare from scratch, even if you think it tastes bland. What may seem bland to you could be perfectly flavorful for your baby. Instead of salt,. try using herbs and spices as to enhance the flavor.
During the first few months of eating, it’s very unlikely that a baby will consume a large amount of sodium, especially if you’re mindful of the foods you provide. Since babies don’t eat that much in the beginning, it’s difficult for them to take in lot of sodium. Additionally, if your baby is self-feeding, it can take time for them to actually ingest a significant amount of food!
As you baby gets older and starts sharing more family-style meals, you’ll need to be more aware of their sodium intake, as hidden sodium can be found in many foods!
AT RESTAURANT
Restaurant foods tend to be much saltier than what you would make at home, and it’s hard to know exactly how much sodium is in a dish. Even if the nutritional information is available, chefs often add salt as they see fit, regardless of the recipe. Here’s how you can approach dining out with your baby.
Generally, I recommend not stressing too much about it. As long as you aren’t eating at a restaurant daily or multiple times a day, it will balance out. Try ordering dishes that are typically prepared with less salt, and don’t hesitate to ask the waiter’s or chef for suggestions.
If your baby isn’t eating much yet, or if they tend to eat small portions, you should be fine. However, if your baby has a good appetite, consider bringing some low-sodium food for home. Personally, I find that I can usually make do with what’s on the menu, and I want my child to experience a variety of flavors. But if you’re unsure, bringing your own is always a good backup.
The key is to be mindful and balance things over the next few days. For example, if one day your baby eat a a lot of cheese and bread, you can focus on offering low or no sodium foods the next day. If they eat a meal at a restaurant, you might serve fruit and a homemade muffin for their next snack.
Pick your battles and make the best choices you can. If you only eat out once or twice a week, just adjust your baby’s food choices for the rest of the week! Keep it truly balanced while continually striving to plan ahead.
BOTTOM LINE
Do your best to serve homemade meals whenever possible. Read labels and be mindful of what you and your baby are eating. This is a healthy habit for the entire family.
What you feed your child today helps shape their taste preferences for the future.
Herbs and spices provide our foods with a multitude of flavours, fragrances, and colours. However, many parents worry about adding flavour this way to their babies’ food, believing that spices are hot and not suitable for little ones’ taste buds.
Baby food doesn’t have to be bland!
There is a big difference between hot spices and aromatic ones. Aromatic spices, such as turmeric, garlic, ginger, dill, cumin, nutmeg, garlic, dill, and cinnamon, are perfectly fine to introduce to baby after 6 months.
This guide explains why I recommend parents adding herbs and spices to baby’s food, the benefits of adding them and gives some ideas on how to start introducing them to your baby.
WHY YOU SHOULD INTRODUCE HERBS AND SPICES TO BABIES
If your baby doesn’t have any digestive problems, I always encourage parents who are just starting weaning their babies, either by purees or baby led weaning (around 6 months of age), to experiment with herbs and spices from the beginning. The more you expose your baby to a variety of tastes and flavours, between 6-12 months, the more likely it is that they’ll accept a variety of food later on in life! This means adding herbs and spices right from the beginning helps reduce the chances of pickiness.
In fact, breastfed babies are often introduced to a variety of spices even before starting solids. Breast milk can change its flavour, depending on a mum’s diet. If mum enjoys spicy and flavoursome food, then her baby will be exposed to this through her milk, helping create and develop a taste for flavoured foods. Therefore, by flavouring food with a variety of herbs and spices, you’ll continue the benefits of flavour exposure found in breastmilk.
What about exclusively formula fed babies? We know that babies are made to handle various flavours from the first day of their life, they were capable of experiencing various spices without any issues. So bland food is actually not a requirement for them and it’s natural for them to experience different flavours. If your baby is exclusively formula fed, then they wouldn’t have that exposure, and so beginning with some herbs and spices when they start solids is a great way to get those taste buds primed for new flavours.
As salt and sugar should be limited in baby food, spices and herbs are a great way to flavour food.
BENEFITS OF INTRODUCING HERBS AND SPICES AT AN EARLY AGE
Trains the baby’s taste buds to enjoy variety flavors and will set the foundation for healthy eating habits.
Teaches the baby to expect change with food. Offering a plain mashed banana one day and a mashed banana with a dash of cinnamon the next can have a valuable influence on the child’s evolving palate.
Fresh herbs are packed with antioxidants, vitamins and minerals.
Herbs and spices are great flavour enhancers without adding unnecessary sugar and salt.
Helps babies transition to family food, as your baby will be familiar with those tastes and more likely to accept them.
WHAT ABOUT HOT SPICY FOODS?
Hot spicy foods (cayenne pepper or jalapeño) can hold off for a while. But, it is recommended to use aromatic spice first, such as curry, cumin, oregano, turmeric, cinnamon, mint, basil, allow them to experience those flavours first, before adding small amounts of hot spices. We live in Malaysia, the 3 major cultures that have influenced Malaysian food are Malay, Chinese and Indian. A lot of Malaysian dishes can be classified under the hot and spicy category. So, once you start, use mild spices in small dosages, therefore, you can cook a dish that the whole family can enjoy.
POPULAR FLAVOUR COMBINATIONS
Here is a list of baby friendly herbs, spices and natural flavor enhancers and the foods that pair well with them:
Vegetables
Asparagus: Parmesan cheese
Banana: rolled in unsweetened coconut
Broccoli: nutritional yeast
Butternut squash: cinnamon, nutmeg, allspice or ginger
Carrots: basil and garlic; or cinnamon
Cauliflower: curry powder
Green beans: garlic powder
Mashed potatoes: dill or garlic
Pumpkin: cinnamon, nutmeg, or ginger
Sweet potato: cardamom, cinnamon, cajun spice or nutmeg
Fruits
Applesauce: cinnamon, nutmeg, allspice, or ginger
Avocado: cilantro or parsley
Bananas: cinnamon or allspice
Pears: ginger or cinnamon
Grains/Cereals
Oatmeal: cinnamon and nutmeg
Pasta: basil, oregano, or garlic
Rice: cinnamon, nutmeg, cardamom, or ginger
Quinoa (sweet): cinnamon, nutmeg, cardamon, or ginger
Quinoa (savory): garlic powder, pepper, onion powder, basil, or oregano
Dairy
Plain yogurt: cinnamon or mint
Meat
Chicken: ginger; rosemary, sage and thyme; lemon zest and pepper; or basil and oregano; paprika
Beef: garlic and pepper; or onion powder and pepper
Salmon: dill, lime or lemon
TIPS TO ADD SPICES & HERBS TO BABY FOOD
When adding herbs and spices, make sure to start simple and try not to add too much so as to overpower the food. Start out by adding one herb or spice to your baby’s food and then building it up from there by mixing with other flavours.
Storage:Store spices in airtight containers away from light and heat. Whole spices will keep for around 1-2 years but after around six months, ground spices will start to lose their aroma and flavour. So buy in small amounts and use often!
Pre-mix spice blends: Always read the packaging when using pre-mix spice blends (as they often have added sugar and salt), try making your own blends.
Start slowly: Start with plain foods so baby can try the taste of the food on its own.
Use small amounts: Once baby has tasted the food plain, you can gradually add spices and herbs you use when cooking for the rest of the family. Use small amounts to start with to allow your baby to get used to different flavours. You don’t want to overpower the food. Start out by adding just a pinch.
Prepare fresh leafy herbsproperly: Wash fresh herbs and then puree or finely mince before adding to baby food. Large leaves can be a choking hazard
Don’t give up: If your baby rejects the flavour of the spices/herbs just remember that it can take up to 10-20 exposures for a new flavour to be accepted.
Let’s give our babies something other than tasteless mush or finger foods to eat! I’m a firm believer that babies deserve the tasty goodness we feed ourselves. When you implement these tips, you will create a change in taste and expectation for your baby. When babies learn to accept change with food, they become less likely to get stuck in food ruts.
If you’ve added herbs and spices to your baby food, what’s your little one’s favourite combinations?







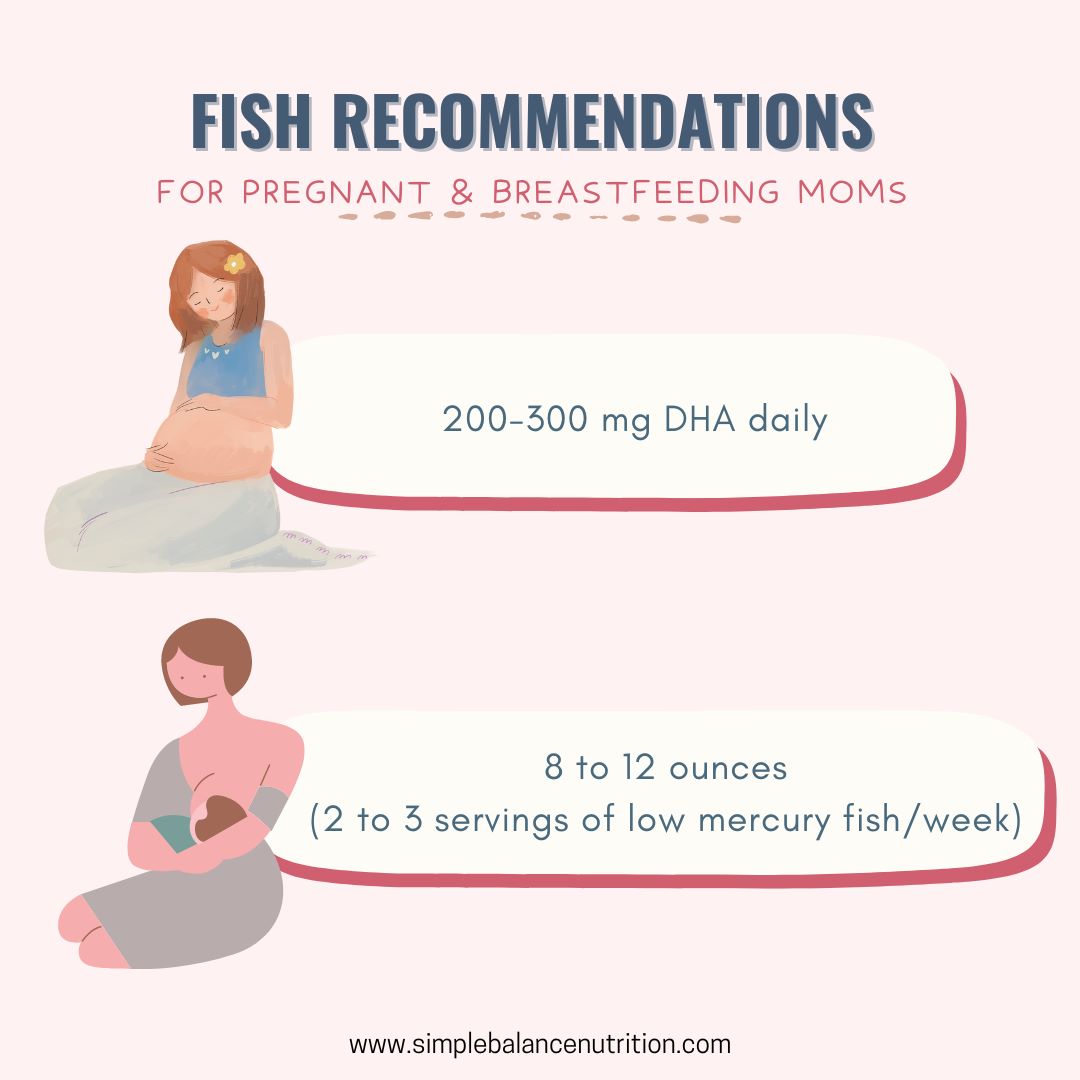
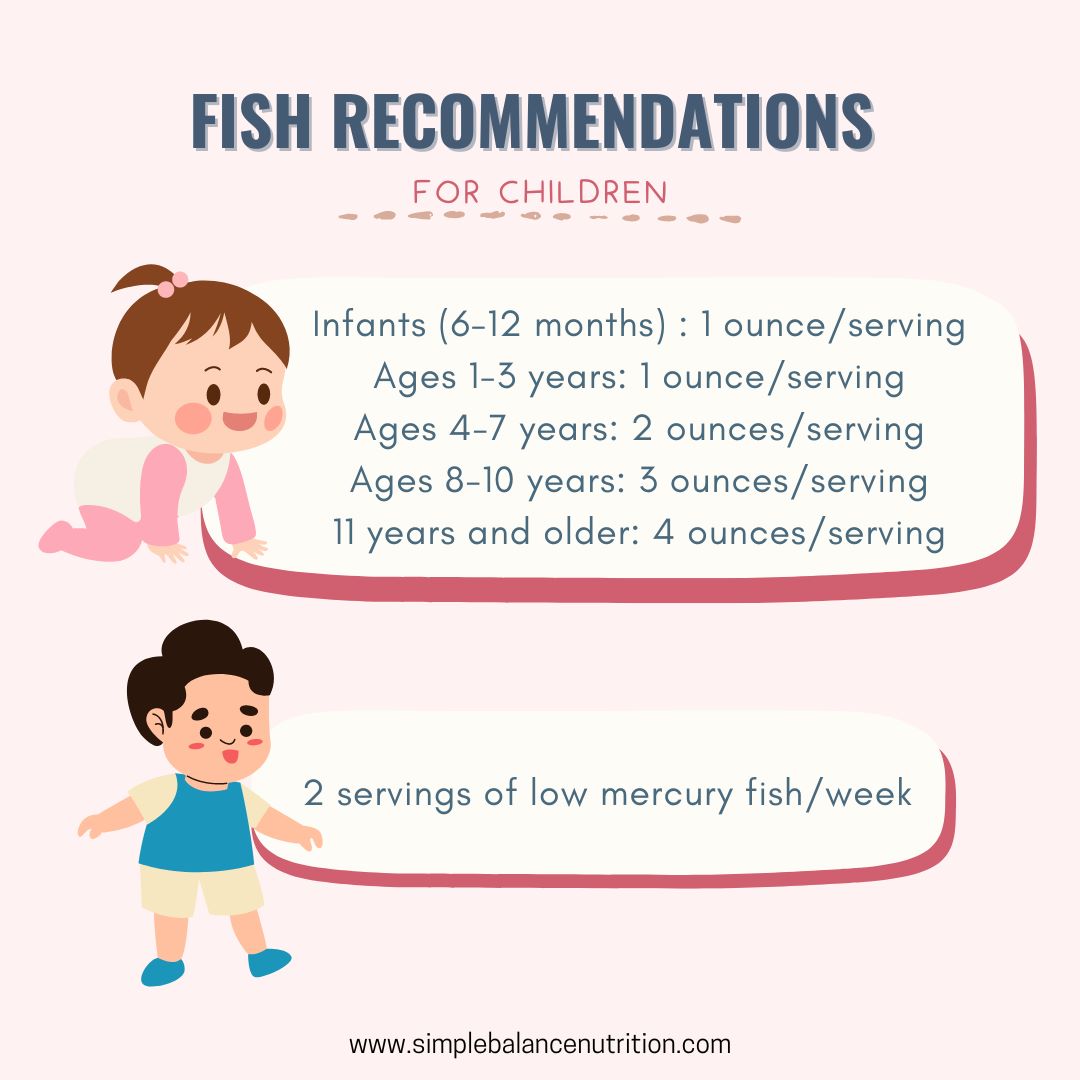
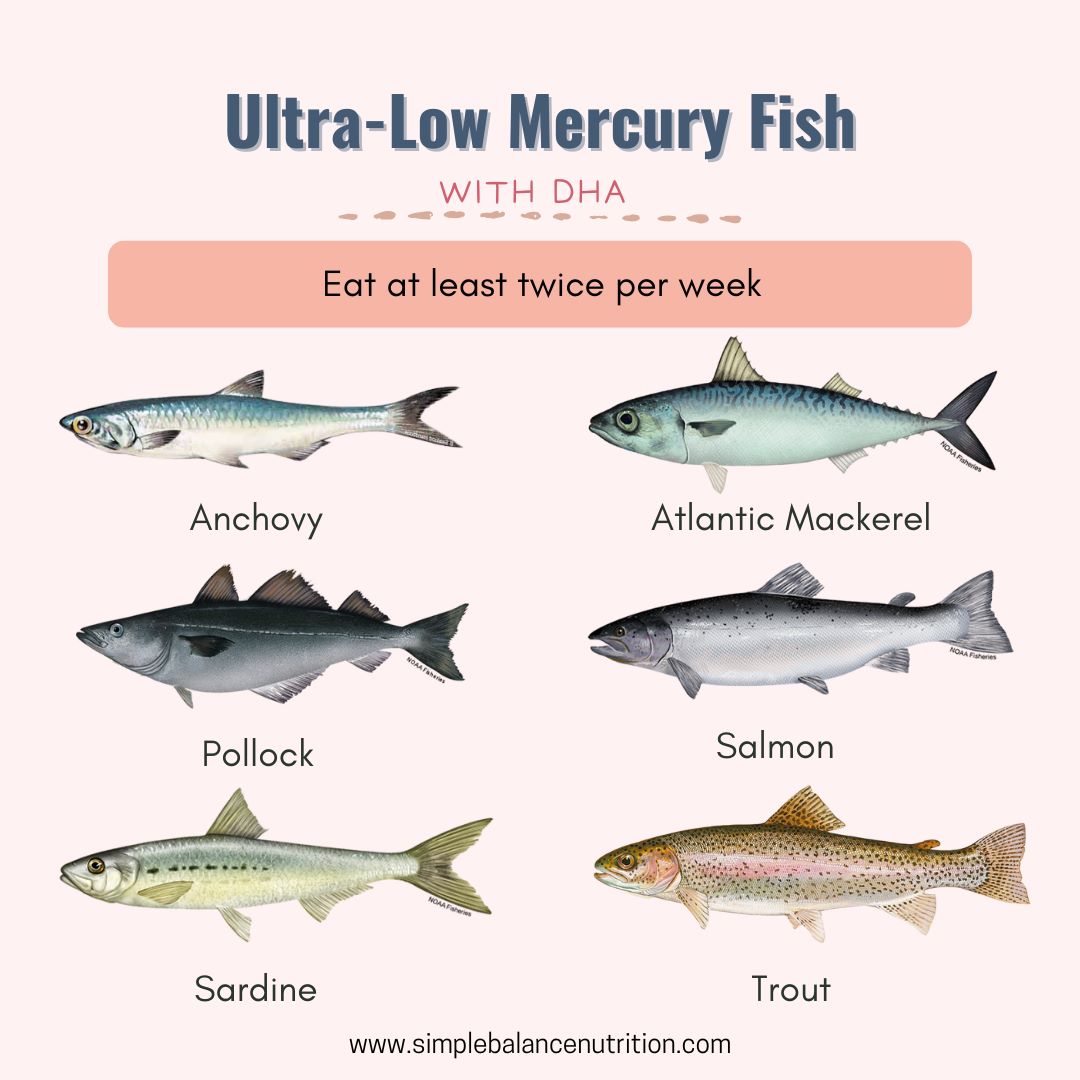





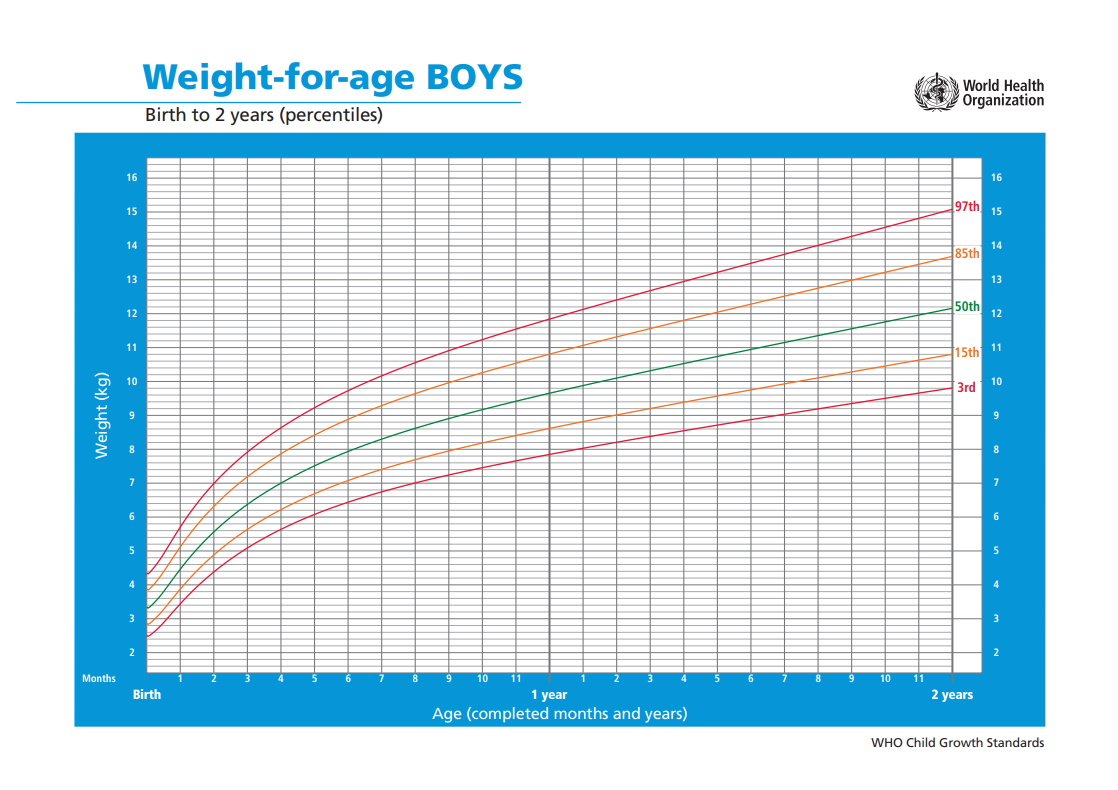
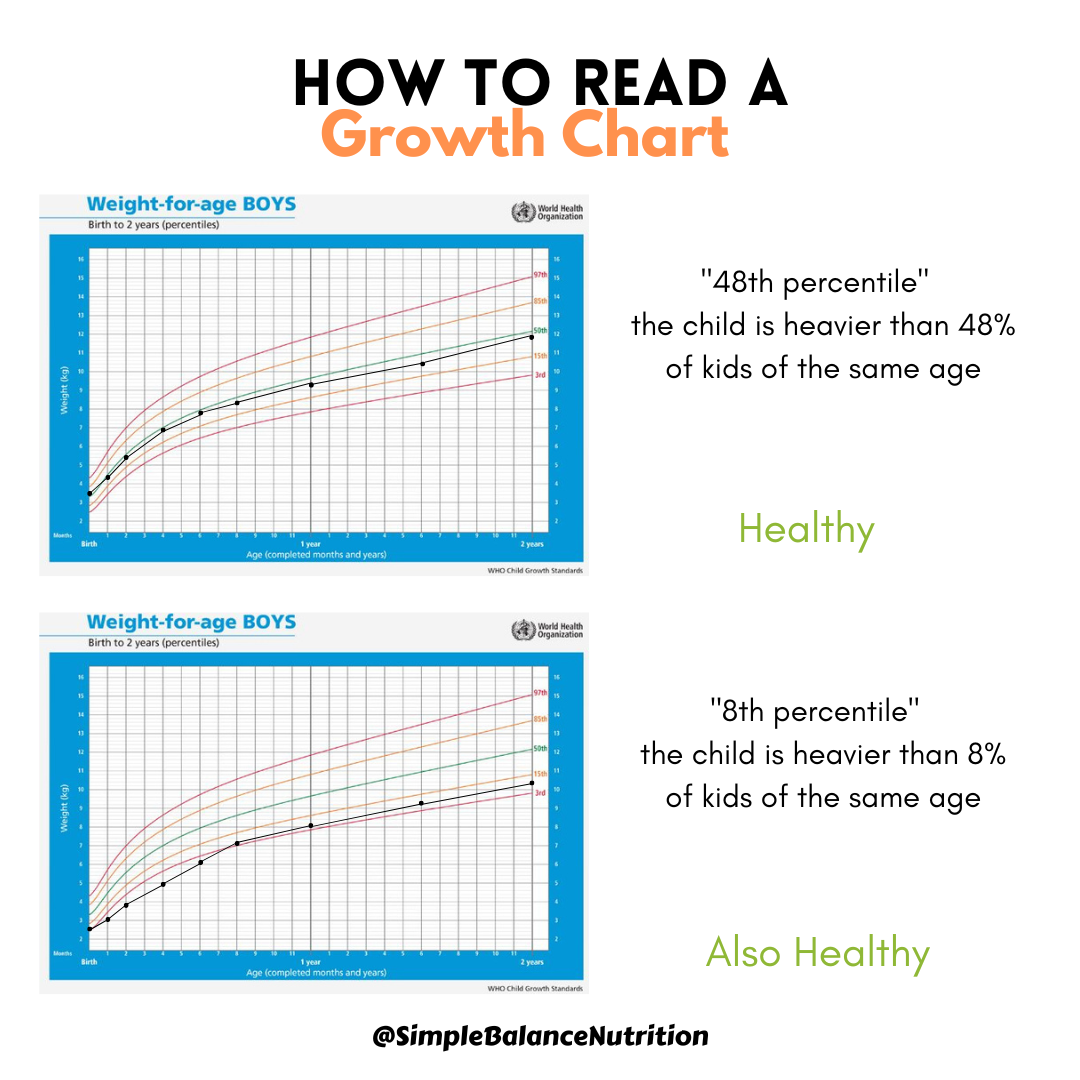
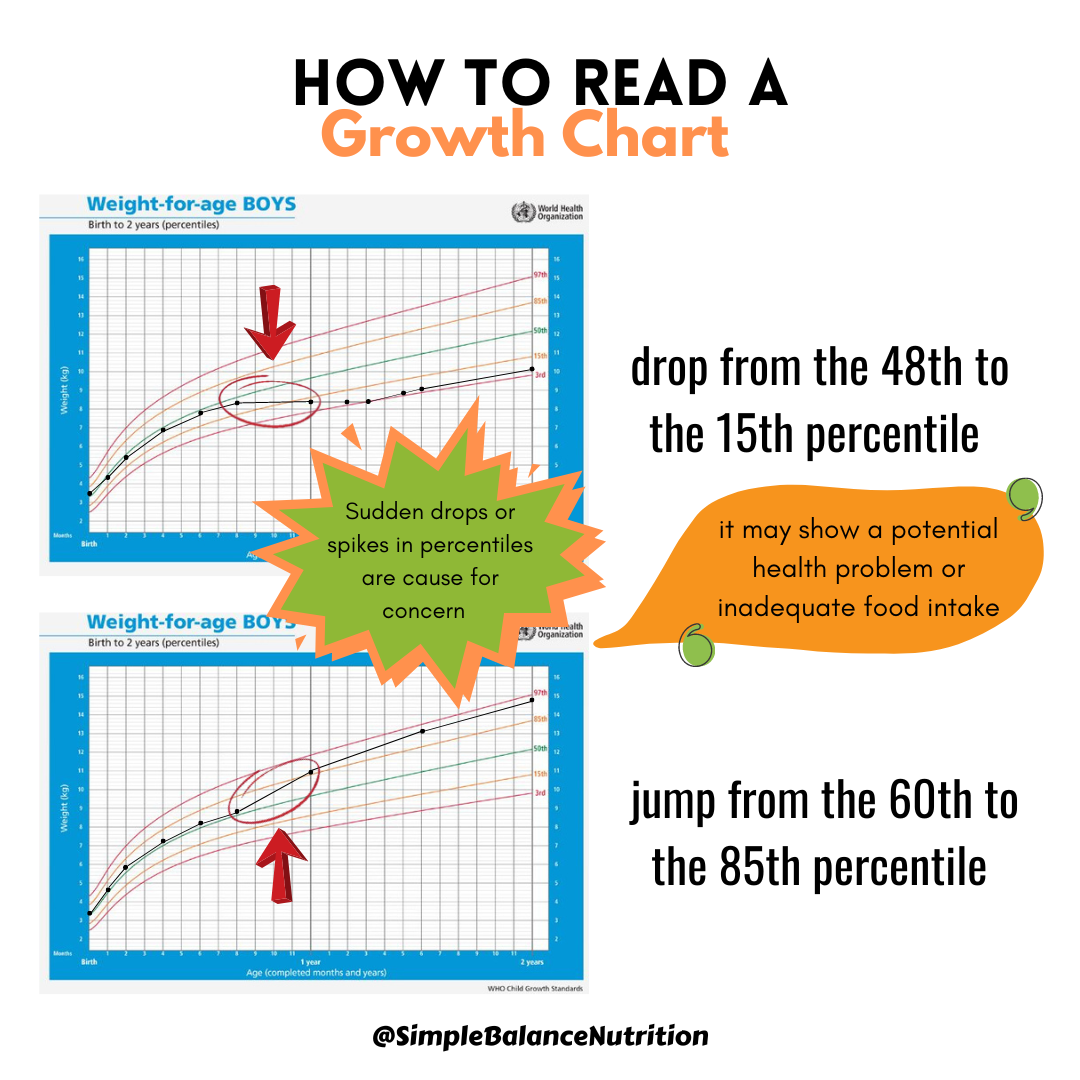
 [/sg_popup]
[/sg_popup]