While I’m a fan of Baby-Led Weaning (BLW), the concern about not getting enough iron intake is real, especially since many moms like to offer fruits and veggies as starter foods for their babies. In fact, this is one of the most common mistakes parents make when practising BLW!
Iron deficiency is estimated to be the most common nutritional deficiency worldwide. It can lead to anemia, impaired growth and development, as well as impaired cognitive function, including delayed attention, learning difficulties and social withdrawal. According to Malaysia’s National Health and Morbidity Survey (NHMS) 2022 Maternal and Child Health report, 46.5% of children between 0-5 years old were anemic. Therefore, contrary to the popular saying, “Food before 1 is just for fun,” the truth is that nutrition in the first year matters greatly.
INCREASED NEEDS

By around 6 months of age, your baby’s iron stores, acquired during pregnancy, begin to deplete. This depletion is influenced by factors such as the mother’s iron levels during gestation, whether cord clamping was delayed at birth, and the baby’s gestational age at birth. In fact, about 80% of a baby’s iron stores are built up during the third trimester of pregnancy, which means that bring born “overdue” can sometimes be an advantages in this context.
While breast milk contains a relatively small amount of iron (about 0.5 mg/L) compared to formula, but the iron present in breast milk is much more bioavailable. Approximately 50% of the iron in breast milk is absorbed, compared to only about 10% from iron-fortified formula. Consequently, both breastfed and formula-fed infants actually end up receiving similar amounts of iron.
By six months, however, babies still obtain some iron from their breast milk or formula, but it is no longer enough to meet their growth needs. This is why the introduction of solid foods becomes crucial, not to replace milk, but to complement it. These first foods are often called “complementary foods,” for this reason.
This leads us to the key question: How much extra iron do babies need, and what are the best food sources to ensure they get enough?
HOW MUCH IRON DOES MY BABY NEED?

So, how much iron does a full-term, healthy-weight baby actually need?
In North America, the Recommended Dietary Allowances (RDA) for iron are:
- BABIES 0-6 MONTHS: 0.27 mg/day*
- BABIES 6-12 MONTHS: 11 mg/day
- TODDLERS 1-3 YEARS: 7 mg/day
* This value is classified as an “Adequate Intake” Instead of a “Recommended Daily Allowance”.
In Malaysia, The Recommended Nutrient Intake (RNI) is slightly different:
- BABIES 6-11 MONTHS: 9 mg/day (assuming 10% bioavailability); or 6 mg/day (assuming 15% bioavailability)
- CHILDREN 1-6 YEARS: 6 mg/day (10% bioavailability); 4 mg/day (15% bioavailability)
So, the exact number depends on which guideline you follow. A practical target is about 7-8 mg of iron daily for 6-12 month olds who consume meat, while vegetarian babies, may need closer to 9-11 mg per day.
It’s important to remember that the RDA of 11mg is an average requirement across 7-12 months, which includes both breastmilk/formula and solid foods. Babies’ iron needs don’t suddenly surge overnight at 6 months. Instead, their requirement rises gradually as they grow.
Naturally, there’s a big difference between a 7-month-old just starting solids and a 12 months-old which can eat a variety of foods. The great news is that babies usually adapt quickly, and with BLW, they can progress to eating a substantial amount of food in just a few months.
Most importantly, you don’t need to tract every milligrams of iron your baby eats, doing so can become stressful and unsustainable. Instead, focus on offering a variety of iron-rich foods consistently throughout the day to help your baby meet their needs.
SIGNS OF IRON DEFICIENCY

If you’re worried that your child isn’t getting enough iron, here are some common signs and symptoms of iron deficiency to look out for:
- Slow weight gain
- Little or no appetite
- Pale skin
- Fatigue or low energy
- Always tired
- Cold hands and feet
- Brittle nails
- Poor immunity (frequent illness or infections)
To help prevent anemia, the American Academy of Pediatrics (AAP) recommends a routine blood test for all 12-month-olds to check iron levels. In Malaysia, if you’ve concerns about your child’s iron intake or notice any of the above signs, it’s advisable to consult a doctor and request a blood test.
If your child’s iron levels are found to be significantly low, iron supplements may be prescribed for a few months. In such cases, diet alone is usually not enough to restore iron levels to normal, and supplementation is necessary under medical supervision.
CAN BABY LED WEANERS GET ENOUGH IRON (RESEARCH)

According to Baby-Led Introduction to Starting SolidS (BLISS) study, two hundred families inNew Zealand were divided into two groups: the BLISS group and the control group.
In the BLISS group, parents were taught to strategies prevent choking, growth faltering, as well as how to ensure an adequate intake of iron-rich foods while self-feeding. They were encouraged to offer at each meal:
- A high iron food (e.g., red meat and fortified cereals)
- An energy-rich food (e.g., cheese or avocado)
- An easy-to-eat food (e.g., fruit or vegetables)
One of the key studies from the BLISS trial, titled “Impact of a Modified Version of Baby-Led Weaning on Iron Intake and Status: A Randomized Controlled Trial,” investigated the outcomes more closely. Researchers assessed nutrient intake at 7 and 12 months using weighted 3-day diet records, and iron status was measured through blood samples taken at 12 months of age.
The results showed that 83% of babies in both the control and BLISS groups had adequate iron levels, while anemia was found in 5% of the control group and 7% of the BLISS group. Importantly, there were no significant differences between the two groups in terms of iron levels and stores at either 7 or 12 months of age.
This is promising news! It suggested that with the right education and guidance, BLW can be a nutritious and safe approach to introducing solid foods without increasing the risk of iron deficiency.
So, Can BLW Babies Get Enough Iron?
The short answer is YES! It is absolutely possible.
Traditionally weaned babies often rely on iron-fortified rice cereal as their main source of iron, which is usually skipped in BLW. But, BLW babies can still meet their iron needs. In fact, BLW babies are often introduced to meat earlier if it’s part of the family’s diet, whereas traditionally weaned babies may not eat meat right away at the beginning of starting solids.
Research shows that as long as parents consistently offer iron-rich foods at each meal, there is no significant difference in the iron status between babies following BLW and those fed purees.
For vegetarian and vegan babies, meeting iron needs may be more challenging, but it is achievable with careful planning. Offering a variety of iron-rich plant-based foods, such as legumes, tofu, leafy greens, and fortified cereals, paired with vitamin C-rich foods to boost absorption, can help ensure adequate intake. In some cases, including fortified rice cereal may also be beneficial.
WHAT FOODS ARE HIGH IN IRON

There are two main types of dietary iron: heme and non-heme.
- Heme iron, found in animal products like meat, fish, and poultry, the human body has a high absorption rates at approximately 20%.
- Non-heme iron, found in plant sources like soy, lentils, beans, and even eggs, but it is less readily absorbed by the body, with only about 10% uptake.
This difference in bioavailability means that not all iron sources are equal.
I don’t believe in focussing too much on numbers or counting exact milligrams of iron every day, as this approach can lead to unnecessary stress. However, I do think it is useful to know the amounts of iron found in realistic serving sizes of some common foods. Here are some examples:
HEME-IRON FOODS (ANIMAL SOURCES):
- Liver (chicken, turkey, lamb), cooked* = 6.2-9.7 mg
- Ground beef (75 g) = 1.3-2.2 mg
- Ground chicken/pork (75 g) = 0.8-1.2 mg
- Chicken (75 g) = 0.4-2 mg (dark meat has higher levels than white meat)
- Sardines, canned (75 g) = 1.7-2.2 mg
- Tuna, light, canned in water (75 g) = 1.2 mg
*While liver is an excellent source of iron, it contains an excessive amount of preformed Vitamin A, which can be toxic for young children. The Upper Limit recommended for ages up to 3 years is 600 micrograms, whereas just 1 oz of liver contains over 5,000 micrograms. Plus, the liver is the filter for our body and may contain trace metals, so it should not be a regular food for babies.
Ways to serve heme-iron foods in BLW:
- Ground meat sauce on pasta or rice
- Mini baby burgers or meatballs
- No-added salt canned sardines as finger food
- Pressure or slow-cooked pork or beef roast, shredded
- Pork ribs or chicken legs (removed skin, gristle and small bones)
- Boneless chicken thighs, cut into finger-sized strips
- Fish or salmon cakes
NON-HEME IRON FOODS (PLANT SOURCES):
- Eggs (2 eggs) – 1.2 – 1.8 mg
- Edamame (1/2 cup) = 1.9-2.4 mg
- Tofu (¾ cup) = 2.4-8 mg
- Lentils (¾ cup) = 4.1-4.9 mg
- Beans (white, kidney, navy, pinto, black, etc.) (¾ cup) = 2.6-4.9 mg
- Hummus (¼ cup) = 1.4 mg
- Oatmeal, instant, cooked (¾ cup) = 4.5-6.6 mg
- Wheat germ (1 tbsp) = 1.2 g
- Spinach, cooked (½ cup) = 2.0 -3.4 mg
- Hemp hearts (1 tbsp) = 1.4 mg
- Blackstrap molasses (1 tbsp) = 3.6 mg
Ways to serve non-heme iron foods in BLW:
- Fried eggs, cut into strips or scrambled
- Firm tofu strips, sautéed or roasted
- Soft tofu blended into smoothies for variety
- Add blackstrap molasses to muffins or pancakes
- Sprinkle wheat germ or hemp hearts onto yogurt or blend into a smoothie
- Spread hummus on a toast fingers
- Offer black beans as finger food for practicing their pincer grasp
- Smush larger beans like chickpeas with your finger, to reduce choking risk
- Bean or lentil patties
- Spread nut butters thinly on toast fingers
TIPS TO GET ENOUGH IRON WHILE USING BLW (6-12 months)

1. Continue offering adequate breast milk or formula as the baby’s main source of nutrients. At this age, solid foods serve as complimentary foods, helping to boost nutrient intake while gradually preparing your baby’s digestive system for the full transition to solids.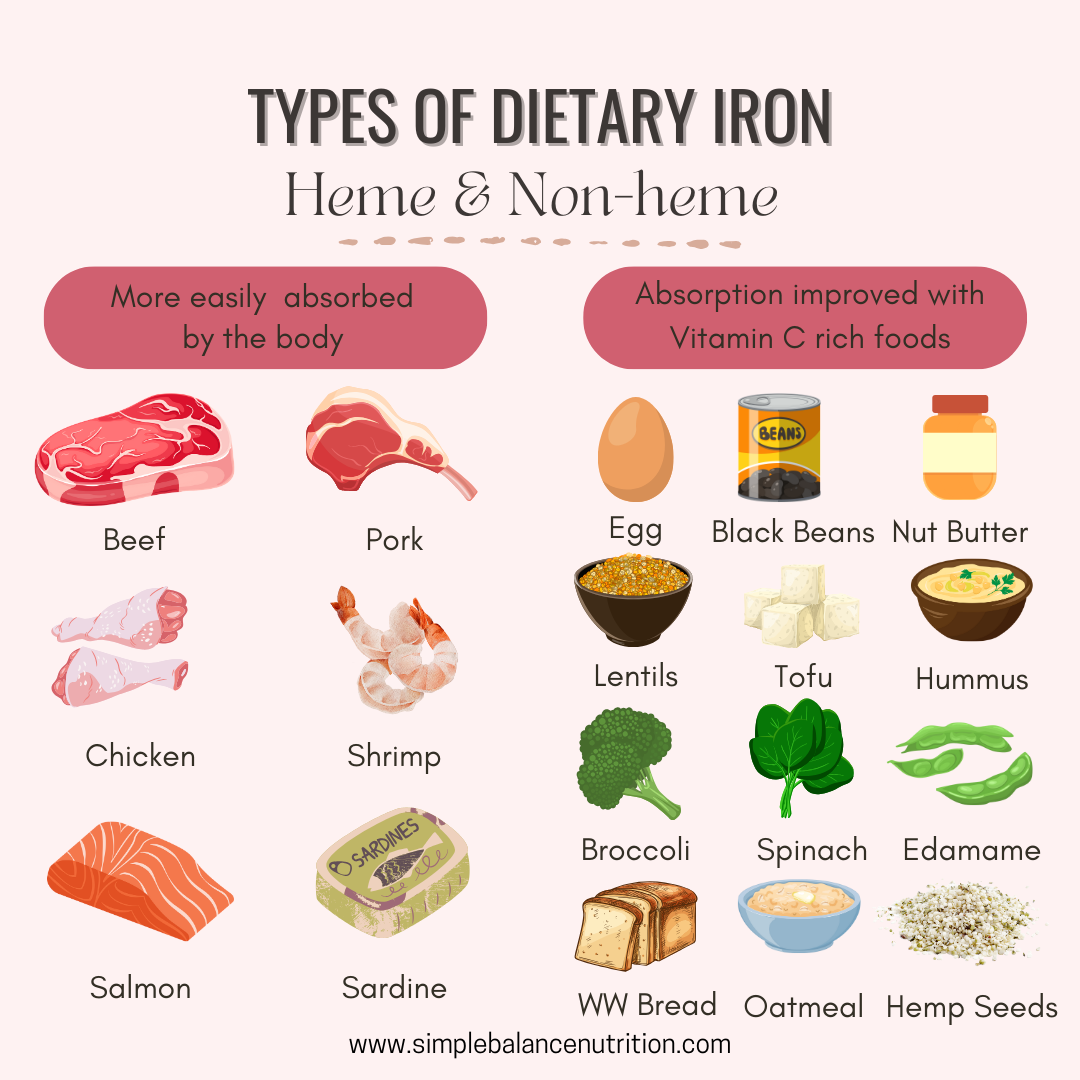
2. Ensure that every meal includes a source of iron, both heme and non-heme iron.
3. Incorporate fortified infant cereal baked into baked finger foods for an easy iron boost. You can also replace half of the flour in pancake recipes with fortified infant cereal to increase iron content.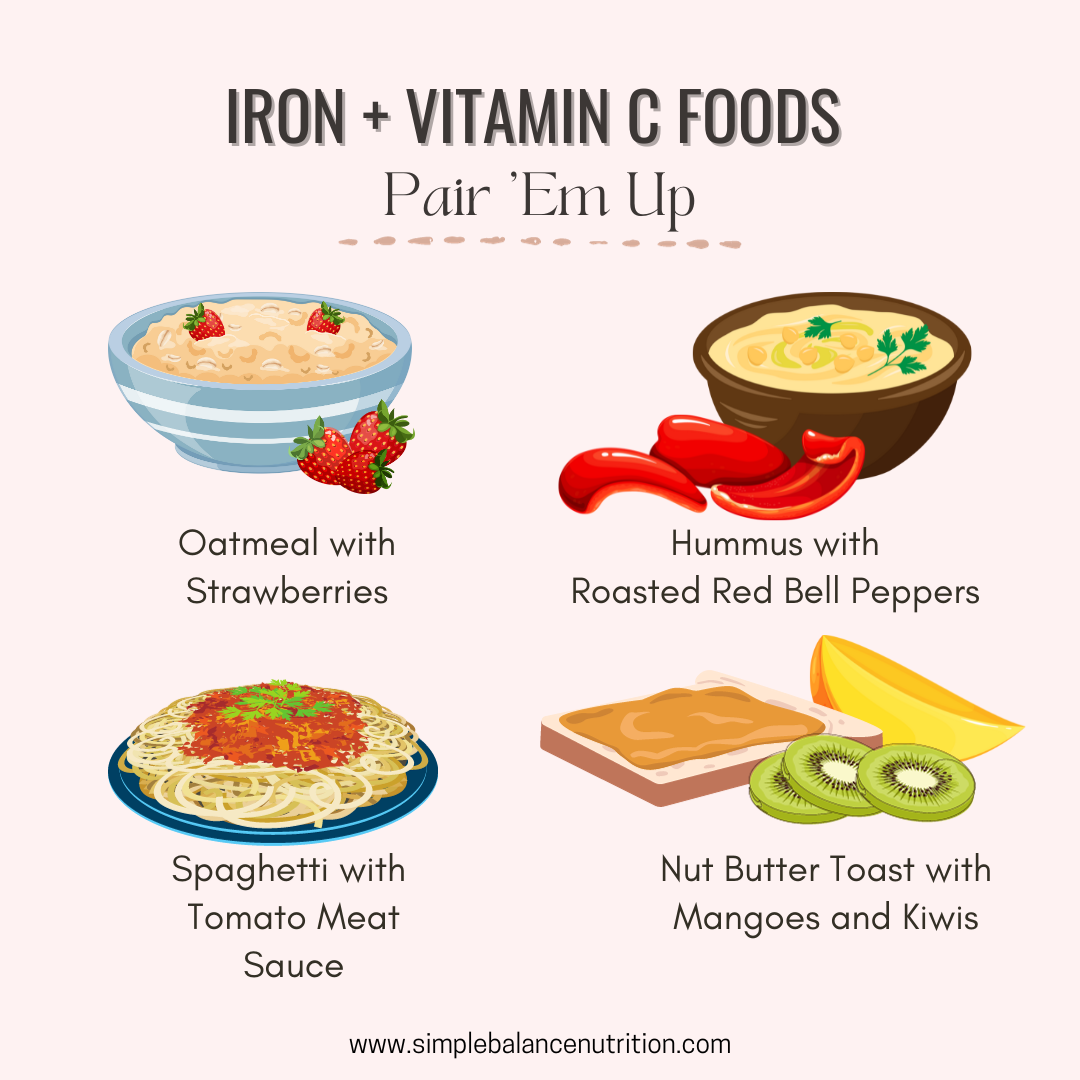
4. Pair iron-rich foods with vitamin C rich foods, to increase the absorption of non-heme iron in the body. For example, top fortified pancakes or cereal with fruit compote; serve lentils in stewed tomatoes and add spinach to a fruit smoothie.
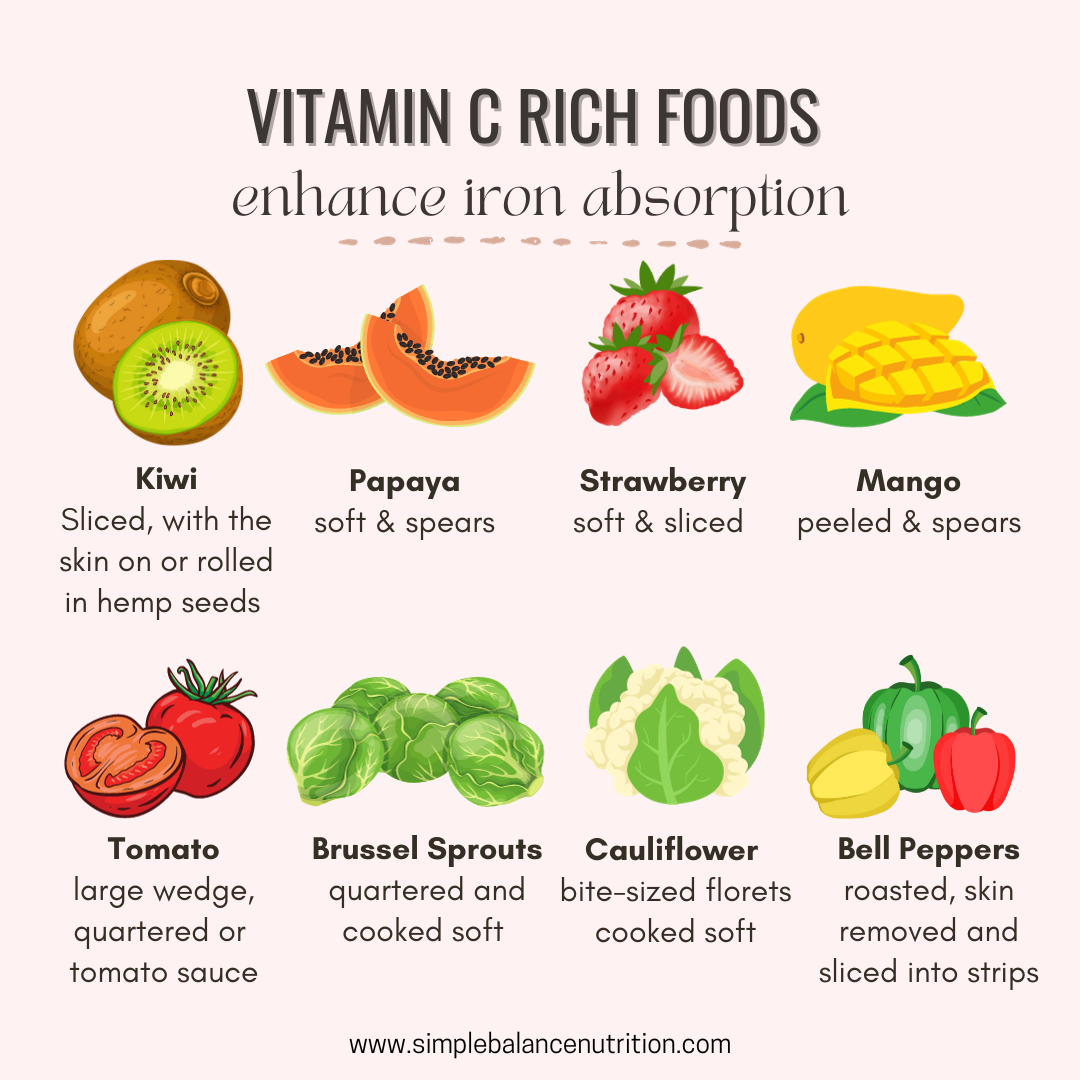
Other excellent sources of vitamin C, including bell peppers, tomatoes, broccoli, citrus fruit and berries, etc. Combing ground meat with a tomato-based sauce creates an ideas meal that provides both heme iron and vitamin C to boost absorption.
5. Cook with cast iron cookware. Cooking with cast-iron pots and pans can safely increase the iron content of your meals. If you don’t have cast-iron cookware, you can try a product called the Lucky Iron Fish®. This simple, reusable and effective cooking tool that adds extra iron to your daily foods, soups or drinks. It is an affordable and effective solution, especially for families managing iron deficiency anemia.
6. Cook with garlic or onion. Preparing meals with allium-containing ingredients, such as garlic and onions can help increase iron absorption.
BOTTOM LINE
Want more tips to make Baby-Led Weaning easier and more enjoyable for your little one? Enroll in our online course, Baby’s First Bites, and get step-by-step guidance to help your baby thrive at mealtimes.
Update: August 19, 2025